Molnupiravir versus placebo in unvaccinated and vaccinated patients with early SARS-CoV-2 infection in the UK (AGILE CST-2): a randomised, placebo-controlled, double-blind, phase 2 trial
Saye H Khoo, Richard Fitzgerald, Geoffrey Saunders, Calley Middleton, Shazaad Ahmad, Christopher J Edwards, Dennis Hadjiyiannakis, Lauren Walker, Rebecca Lyon, Victoria Shaw, Pavel Mozgunov, Jimstan Periselneris, Christie Woods, Katie Bullock, Colin Hale, Helen Reynolds, Nichola Downs, Sean Ewings, Amanda Buadi, David Cameron, Thomas Edwards, Emma Knox, I'ah Donovan-Banfield, William Greenhalf, Justin Chiong, Lara Lavelle-Langham, Michael Jacobs, Josh Northey, Wendy Painter, Wayne Holman, David G Lalloo, Michelle Tetlow, Julian A Hiscox, Thomas Jaki, Thomas Fletcher, Gareth Griffiths, Nicholas Paton, Fred Hayden, Janet Darbyshire, Amy Lucas, Ulrika Lorch, Andrew Freedman, Richard Knight, Stevan Julious, Rachel Byrne, Ana Cubas Atienzar, Jayne Jones, Chris Williams, Anna Song, Jan Dixon, Anja Alexandersson, Parys Hatchard, Emma Tilt, Andrew Titman, Ale Doce Carracedo, Vatsi Chandran Gorner, Andrea Davies, Louis Woodhouse, Nicola Carlucci, Emmanuel Okenyi, Marcin Bula, Kate Dodd, Jennifer Gibney, Lesley Dry, Zalina Rashid Gardner, Amin Sammour, Christine Cole, Tim Rowland, Maria Tsakiroglu, Vincent Yip, Rostam Osanlou, Anna Stewart, Ben Parker, Tolga Turgut, Afshan Ahmed, Kay Starkey, Sujamole Subin, Jennifer Stockdale, Lisa Herring, Jonathon Baker, Abigail Oliver, Mihaela Pacurar, Dan Owens, Alistair Munro, Gavin Babbage, Saul Faust, Matthew Harvey, Danny Pratt, Deepak Nagra, Aashish Vyas
The Lancet Infectious Diseases, doi:10.1016/s1473-3099(22)00644-2
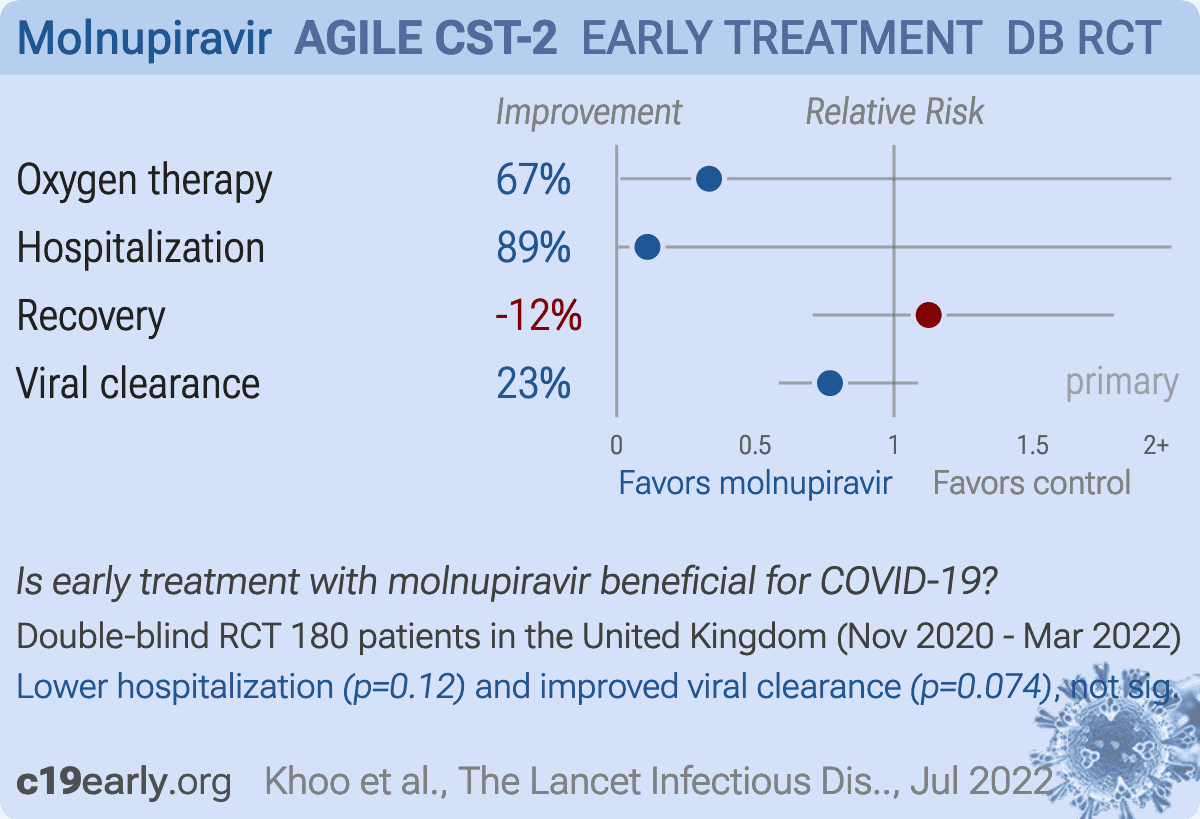
Background The antiviral drug molnupiravir was licensed for treating at-risk patients with COVID-19 on the basis of data from unvaccinated adults. We aimed to evaluate the safety and virological efficacy of molnupiravir in vaccinated and unvaccinated individuals with COVID-19. Methods This randomised, placebo-controlled, double-blind, phase 2 trial (AGILE CST-2) was done at five National Institute for Health and Care Research sites in the UK. Eligible participants were adult (aged ≥18 years) outpatients with PCR-confirmed, mild-to-moderate SARS-CoV-2 infection who were within 5 days of symptom onset. Using permuted blocks (block size 2 or 4) and stratifying by site, participants were randomly assigned (1:1) to receive either molnupiravir (orally; 800 mg twice daily for 5 days) plus standard of care or matching placebo plus standard of care.
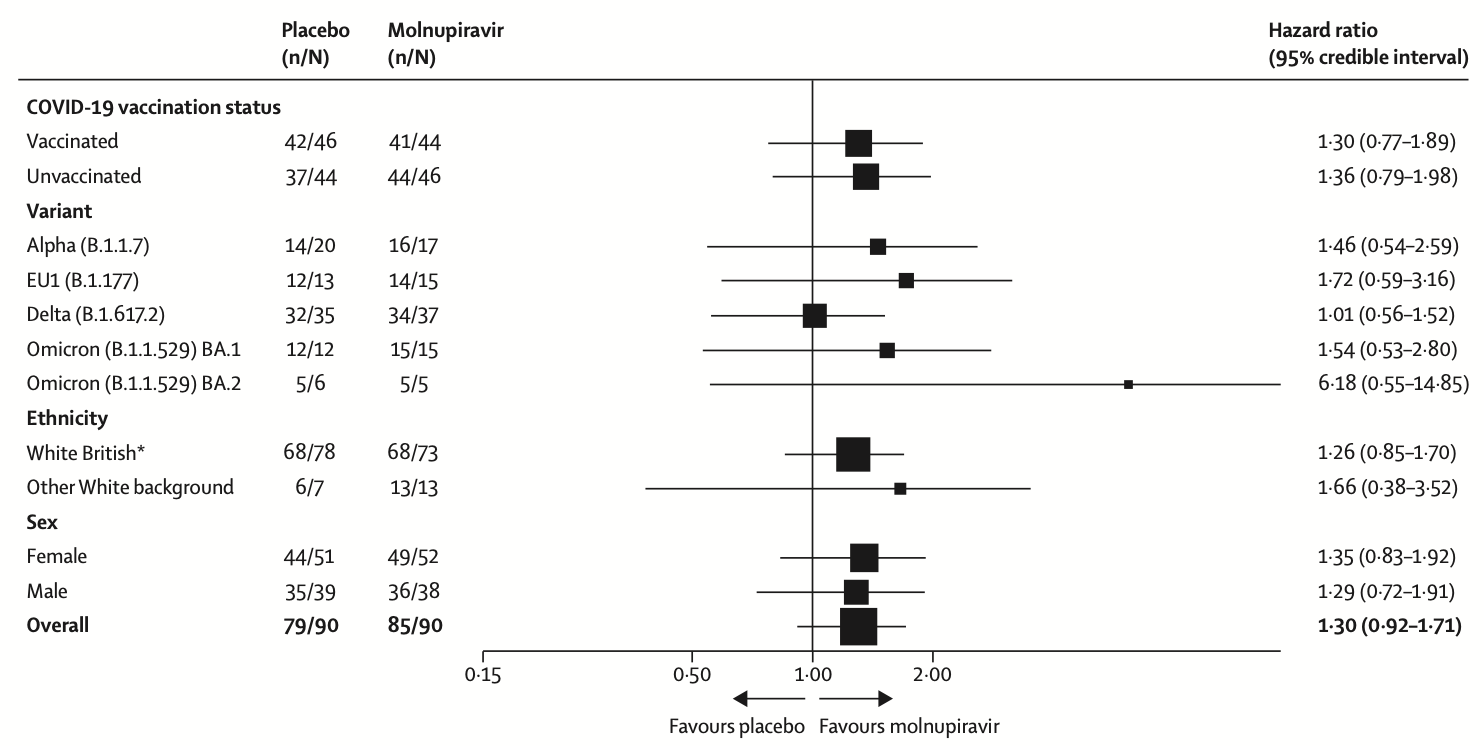
The primary outcome was the time from randomisation to SARS-CoV-2 PCR negativity on nasopharyngeal swabs and was analysed by use of a Bayesian Cox proportional hazards model for estimating the probability of a superior virological response (hazard ratio [HR]>1 ) for molnupiravir versus placebo. Our primary model used a two-point prior based on equal prior probabilities (50%) that the HR was 1•0 or 1•5. We defined a priori that if the probability of a HR of more than 1 was more than 80% molnupiravir would be recommended for further testing. The primary outcome was analysed in the intention-to-treat population and safety was analysed in the safety population, comprising participants who had received at least one dose of allocated treatment. This trial is registered in ClinicalTrials.gov, NCT04746183, and the ISRCTN registry, ISRCTN27106947, and is ongoing.
(199 grade 1-2 and one grade ≥3) in the molnupiravir group and 219 adverse events (211 grade 1-2 and eight grade ≥3) in the placebo group. One participant in the molnupiravir group (grade 3 hypertension) and three participants in the placebo group (eight events; grade 3
Discussion Molnupiravir received conditional marketing authorisation from the UK Medicines and Healthcare products Regulatory Agency and early use authorisation from the US Food and Drug Administration on the basis of data from the MOVe-OUT study 2 in unvaccinated individuals at high risk of severe disease who were infected with the SARS-CoV-2 variants in circulation between May and October, 2021. 2 MOVe-OUT found that molnupiravir had good tolerability and reduced the number of hospitalisations and deaths by about 50% at the interim evaluation, falling to around 30% after all 1433 patients had been analysed. An evaluation of the effect of molnupiravir on virological response by SARS-CoV-2 variant or in vaccinated patients within a randomised controlled trial has not been previously published. In our phase 2 study, patients in the molnupiravir group had a faster median time from randomisation to PCR negativity than did patients in the placebo group. We used a Bayesian framework to facilitate decision making. Using a two-point prior approach, the probability of the HR for PCR negativity being more than 1 (ie, in favour of molnupiravir vs placebo) was 75•4%, which was less than the 80% threshold we had set..
References
Bernal, Da Silva, Musungaie, Molnupiravir for oral treatment of Covid-19 in nonhospitalized patients, N Engl J Med
Coolen, Wolters, Tostmann, SARS-CoV-2 wholegenome sequencing using reverse complement PCR: for easy, fast and accurate outbreak and variant analysis, J Clin Virol
Ewings, Saunders, Jaki, Mozgunov, Practical recommendations for implementing a Bayesian adaptive phase I design during a pandemic, BMC Med Res Methodol
Griffiths, Fitzgerald, Jaki, AGILE: a seamless phase I/ IIa platform for the rapid evaluation of candidates for COVID-19 treatment: an update to the structured summary of a study protocol for a randomised platform trial letter, Lancet Infect Dis
He, Lau, Wu, Temporal dynamics in viral shedding and transmissibility of COVID-19, Nat Med
Khoo, Fitzgerald, Fletcher, Optimal dose and safety of molnupiravir in patients with early SARS-CoV-2: a phase I, openlabel, dose-escalating, randomized controlled study, J Antimicrob Chemother
Kumarasamy, Saha, Jindal, Phase 3 trial of molnupiravir in adults with mild SARS-CoV-2 infection in India, Conference on Retroviruses and Opportunistic Infections
O'toole, Scher, Underwood, Assignment of epidemiological lineages in an emerging pandemic using the Pangolin tool, Virus Evol
Troth, Butterton, Deanda, Letter to the editor in response to Zhou et al, J Infect Dis
Wong, Au, Lau, Lau, Cowling et al., Real-world effectiveness of early molnupiravir or nirmatrelvirritonavir in hospitalised patients with COVID-19 without supplemental oxygen requirement on admission during Hong Kong's omicron BA.2 wave: a retrospective cohort study, Lancet Infect Dis,
doi:10.1016/S1473-3099(22)00507-2

{kind=link}
{kind=link}