


Sleep for COVID-19: real-time meta analysis of 15 studies
Abstract
Statistically significant lower risk is seen for mortality, hospitalization, and cases. 12 studies from 12 independent teams in 5 countries show statistically significant
improvements.
Meta analysis using the most serious outcome reported shows
30% [22‑38%] lower risk. Results are similar for peer-reviewed studies.
Results are robust — in exclusion sensitivity analysis 13 of 15
studies must be excluded to avoid finding statistically significant efficacy
in pooled analysis.
Studies analyze sleep quality before infection, and use different definitions of sleep quality.
No treatment or intervention
is 100% effective. All practical, effective, and safe means should be used
based on risk/benefit analysis.
All data to reproduce this paper and
sources are in the appendix.
{kind=link}
Highlights
Good quality sleep reduces
risk for COVID-19 with very high confidence for mortality, hospitalization, cases, and in pooled analysis.
15th treatment shown effective with ≥3 clinical studies in
March 2021, now with p = 0.0000000019 from 15 studies.
Real-time updates and corrections,
transparent analysis with all results in the same format, consistent protocol
for 69
treatments, outcome specific analyses and combined evidence from all studies.
{kind=link}
{kind=link}
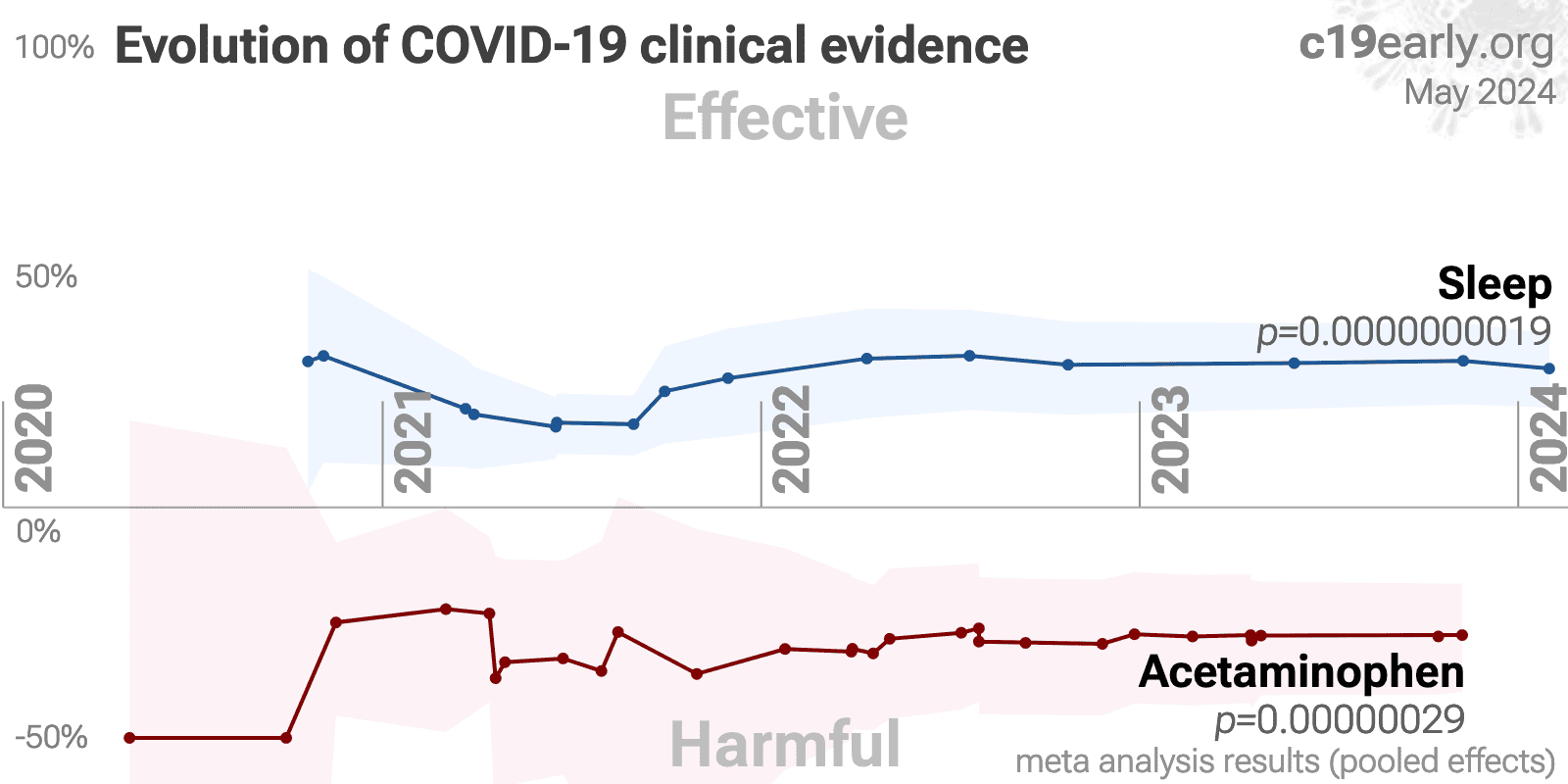
Figure 1.
A. Random effects
meta-analysis. This plot shows pooled effects,
see the specific outcome analyses for individual outcomes.
Analysis validating pooled outcomes for
COVID-19 can be found below.
Effect extraction is pre-specified, using the most serious outcome reported.
For details see the appendix.
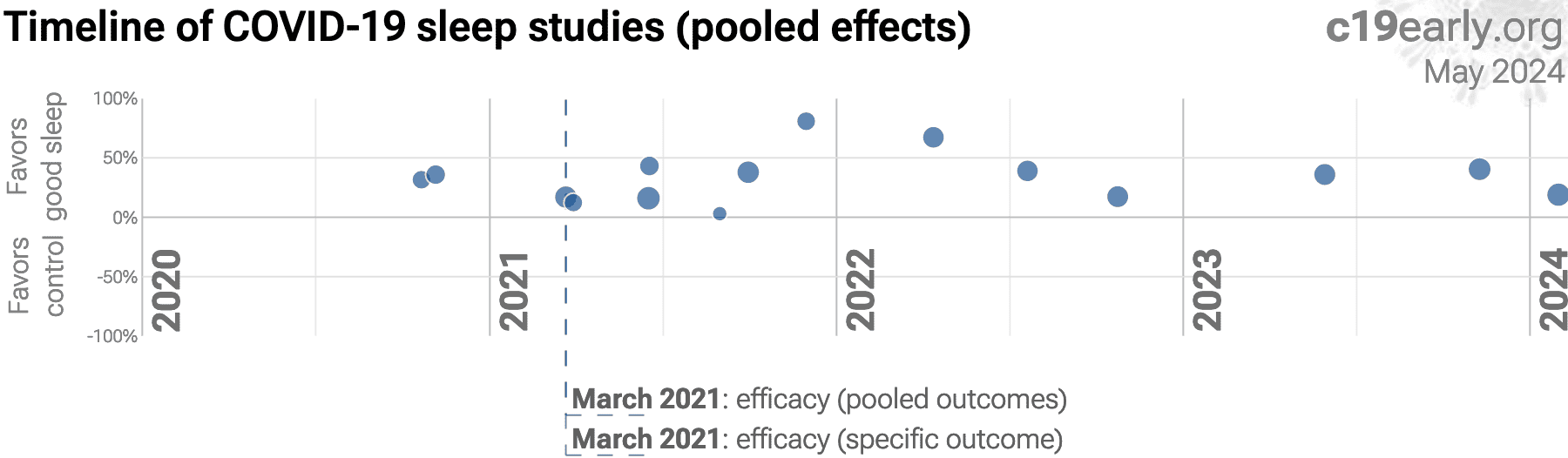
B. Timeline of results in sleep studies. The marked dates indicate the time when efficacy was known with a statistically significant improvement of ≥10% from ≥3 studies for pooled outcomes and one or more specific outcome.
Sleep can improve the absorption, metabolism, and utilization of nutrients, reduce chronic inflammation, improve cardiovascular health, improve comorbidities, and reduce stress. Sleep is crucial for the proper functioning of the immune system. During sleep, the body produces and releases cytokines and T cells that help fight infections, reduce inflammation, and create immune memory.
We analyze all significant
studies reporting COVID-19 outcomes as a function of sleep quality and providing adjusted results.
Search methods, inclusion criteria, effect extraction criteria (more serious
outcomes have priority), all individual study data, PRISMA answers, and
statistical methods are detailed in Appendix 1. We present random
effects meta-analysis results for all studies, individual outcomes, and peer-reviewed studies.
Table 1 summarizes the results for all studies, for peer-reviewed studies, and for specific outcomes.
Figure 2, 3, 4, 5, and 6
show forest plots for random effects meta-analysis of
all studies with pooled effects, mortality results, hospitalization, cases, and peer reviewed studies.
| Improvement | Studies | Patients | Authors | |
|---|---|---|---|---|
| All studies | 30% [22‑38%] **** | 15 | 429,001 | 146 |
| Peer-reviewed studiesPeer-reviewed | 29% [20‑37%] **** | 13 | 358,294 | 134 |
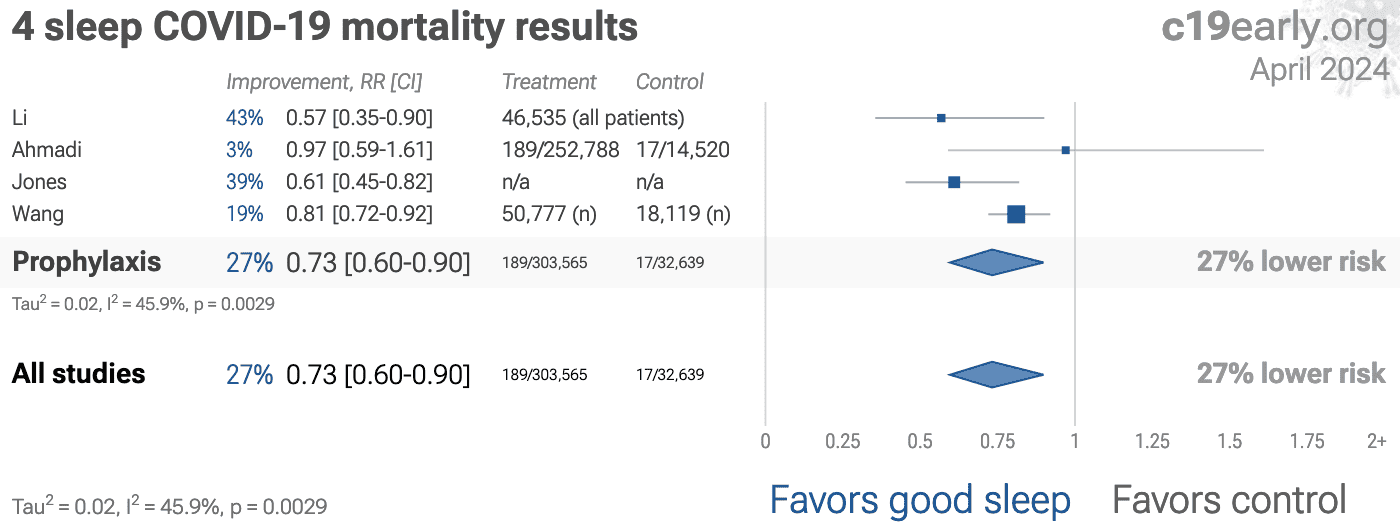
| Mortality | 27% [10‑40%] ** | 4 | 382,739 | 35 |
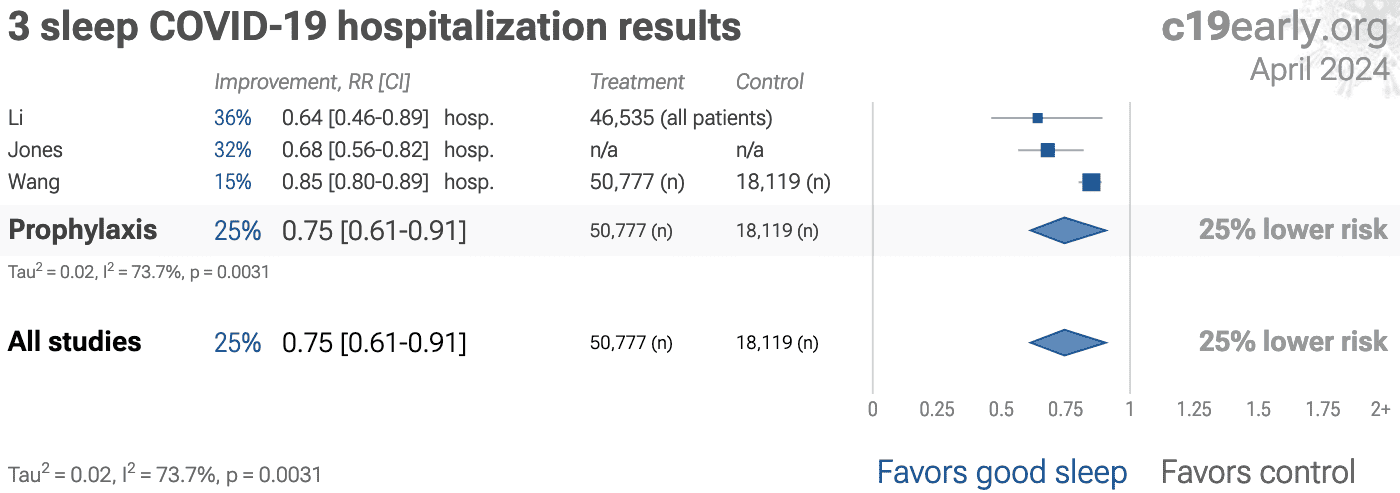
| HospitalizationHosp. | 25% [9‑39%] ** | 3 | 115,431 | 30 |
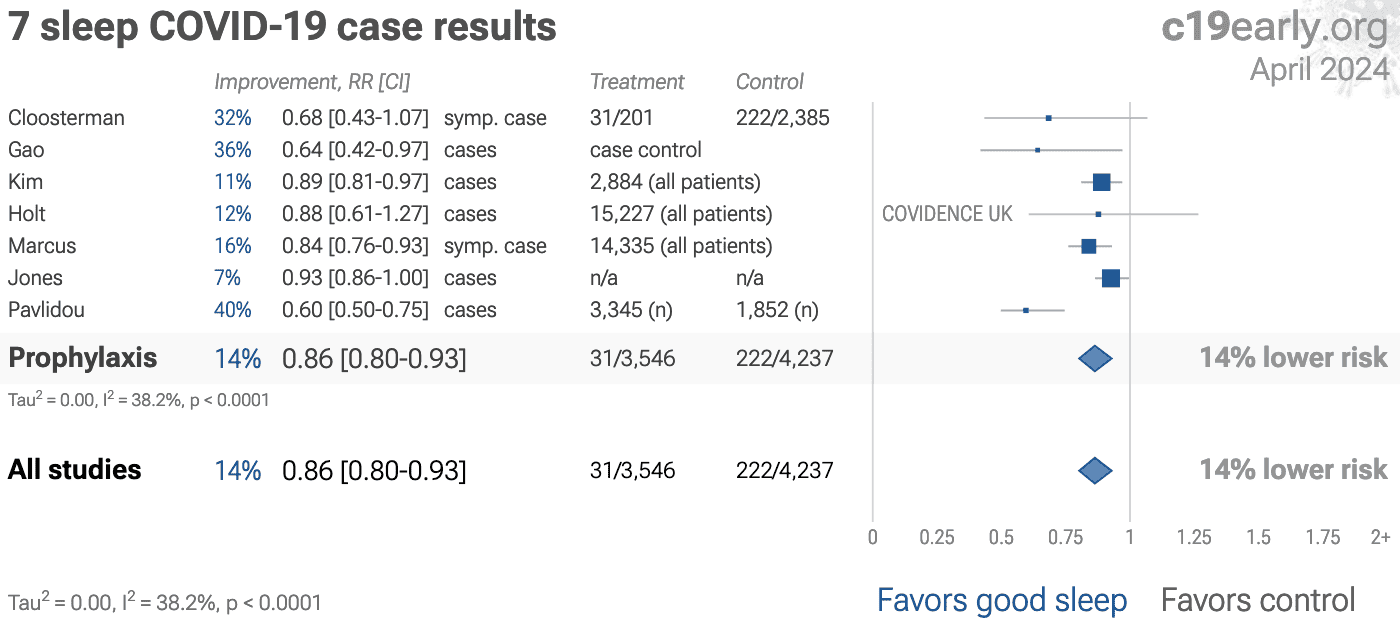
| Cases | 14% [7‑20%] **** | 7 | 40,229 | 95 |
Loading..
Loading..
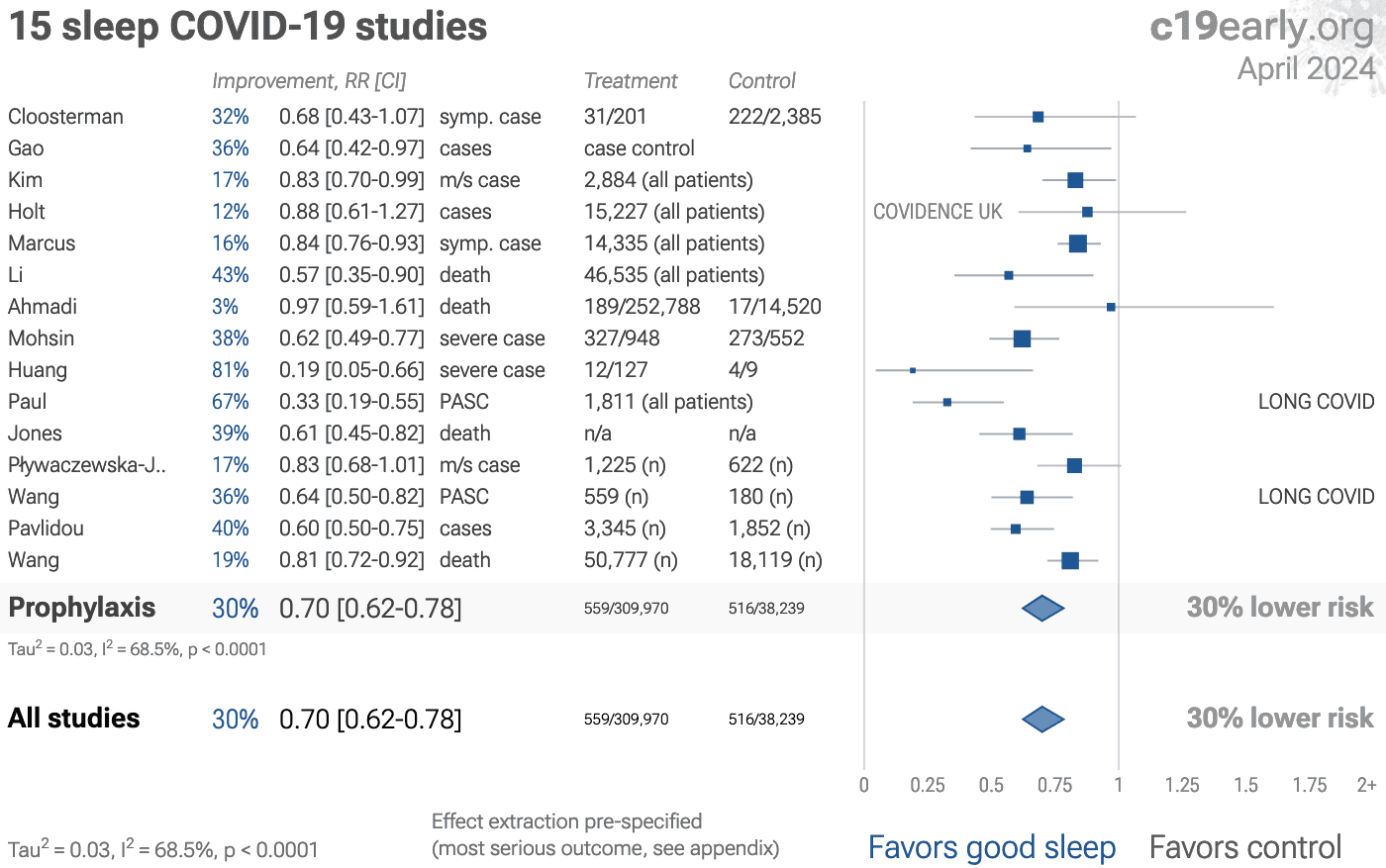
Figure 2. Random effects meta-analysis for all studies.
This plot shows pooled effects,
see the specific outcome analyses for individual outcomes.
Analysis validating pooled outcomes for
COVID-19 can be found below.
Effect extraction is pre-specified, using the most serious outcome reported.
For details see the appendix.
{kind=link}
Loading..
Loading..
Figure 3. Random effects meta-analysis for mortality results.
{kind=link}
Loading..
Figure 4. Random effects meta-analysis for hospitalization.
{kind=link}
Loading..
Figure 5. Random effects meta-analysis for cases.
{kind=link}
Loading..
Figure 6. Random effects meta-analysis for peer reviewed studies.
Effect extraction is pre-specified, using the most serious outcome reported,
see the appendix for details.
Analysis validating pooled outcomes for
COVID-19 can be found below.
Zeraatkar et al. analyze 356 COVID-19 trials, finding no significant
evidence that preprint results are inconsistent with peer-reviewed studies.
They also show extremely long peer-review delays, with a median of 6 months to
journal publication. A six month delay was equivalent to around 1.5 million
deaths during the first two years of the pandemic. Authors recommend using
preprint evidence, with appropriate checks for potential falsified data, which
provides higher certainty much earlier. Davidson et al. also showed no
important difference between meta analysis results of preprints and
peer-reviewed publications for COVID-19, based on 37 meta analyses including
114 trials.
For COVID-19, delay in clinical results translates into
additional death and morbidity, as well as additional economic and societal
damage. Combining the results of studies reporting different outcomes is
required.
There may be no mortality in a trial with low-risk patients,
however a reduction in severity or improved viral clearance may translate
into lower mortality in a high-risk population.
Different studies may report lower severity, improved recovery, and lower mortality,
and the significance may be very high when combining the results.
"The studies reported different outcomes"
is not a good reason for disregarding results.
We present both specific outcome and pooled analyses.
In order to combine the results of studies reporting different outcomes we use
the most serious outcome reported in each study, based on the thesis that
improvement in the most serious outcome provides comparable measures of
efficacy for a treatment. A critical advantage of this approach is
simplicity and transparency.
There are many other ways to combine evidence for different outcomes, along
with additional evidence such as dose-response relationships, however these
increase complexity.
Another way to view pooled analysis is that we are using more of
the available information. Logically we should, and do, use additional
information. For example dose-response and
treatment delay-response relationships provide significant additional evidence
of efficacy that is considered when reviewing the evidence for a
treatment.
Trials with high-risk patients may be restricted due to ethics for treatments
that are known or expected to be effective, and they increase difficulty for
recruiting. Using less severe outcomes as a proxy for more serious outcomes
allows faster collection of evidence.
For many COVID-19 treatments, a reduction in mortality logically
follows from a reduction in hospitalization, which follows from a reduction in
symptomatic cases, which follows from a reduction in PCR positivity. We can
directly test this for COVID-19.
Analysis of the the association between different outcomes across studies from
all 69
treatments we cover confirms the validity of pooled outcome analysis for COVID-19.
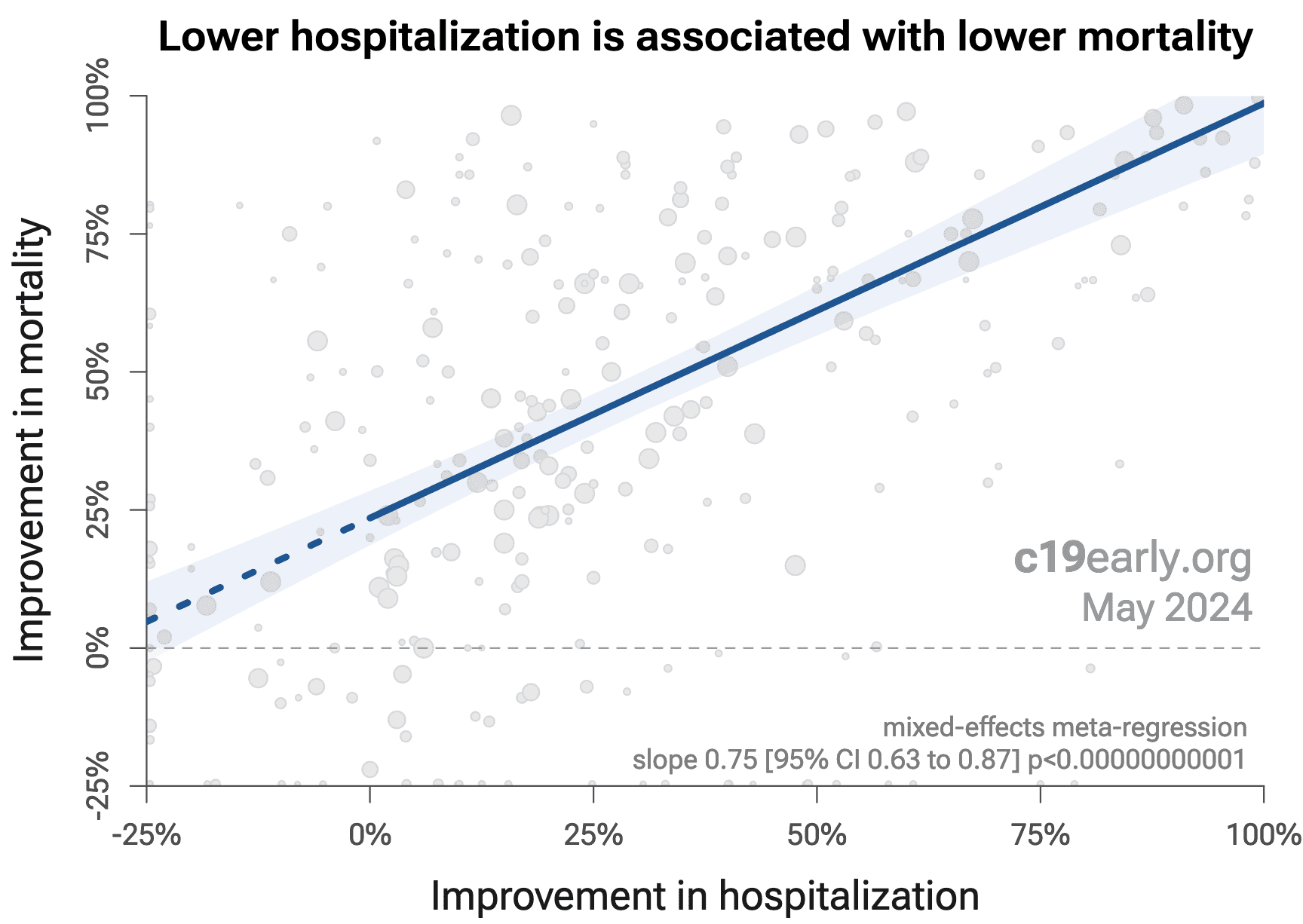
Figure 7 shows that lower hospitalization is very strongly associated
with lower mortality (p < 0.000000000001).
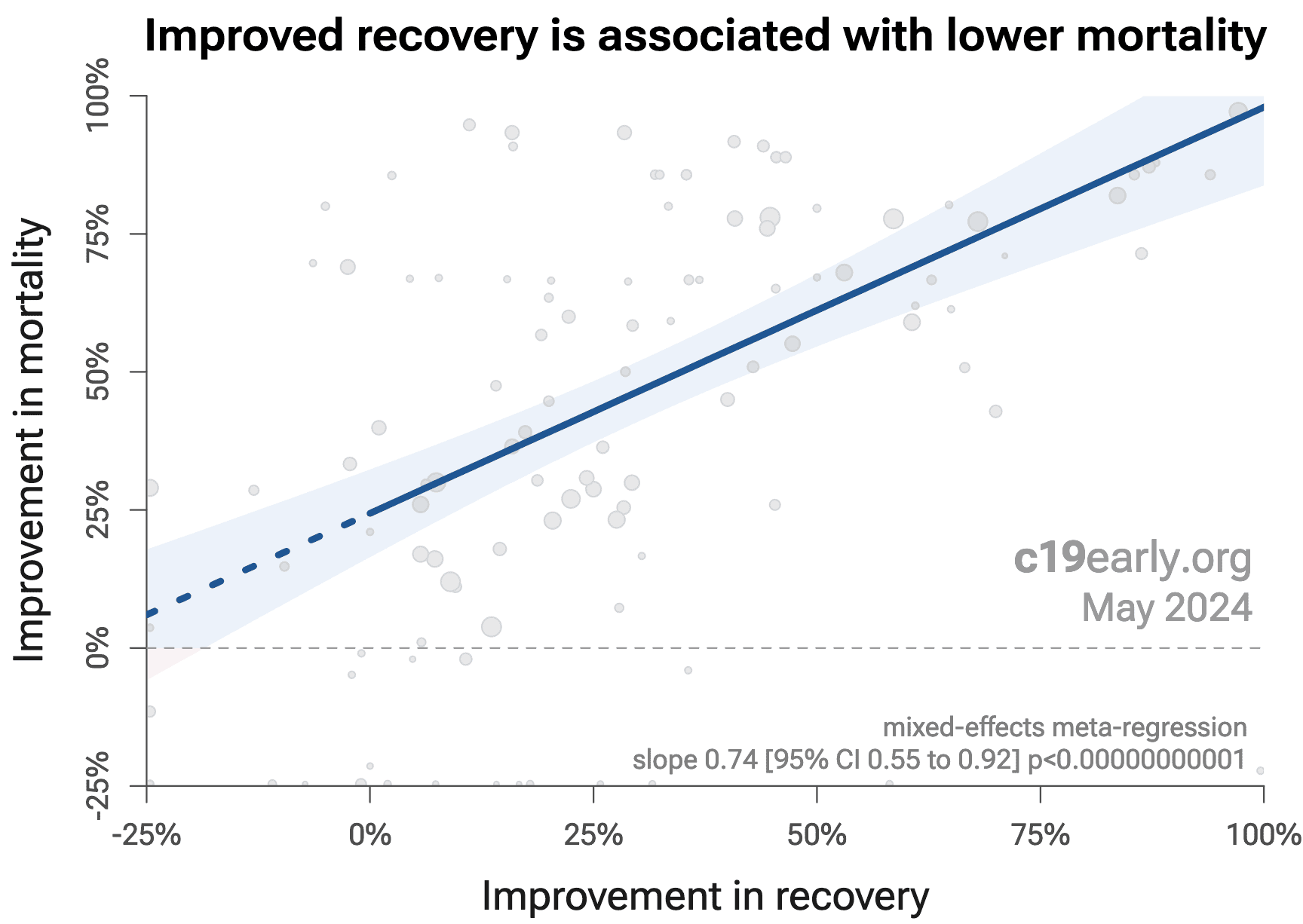
Similarly, Figure 8 shows that improved recovery is very strongly associated
with lower mortality (p < 0.000000000001).
Considering the extremes, Singh et al. show an association between viral clearance and
hospitalization or death, with p = 0.003 after excluding one large
outlier from a mutagenic treatment, and based on 44 RCTs including 52,384
patients.
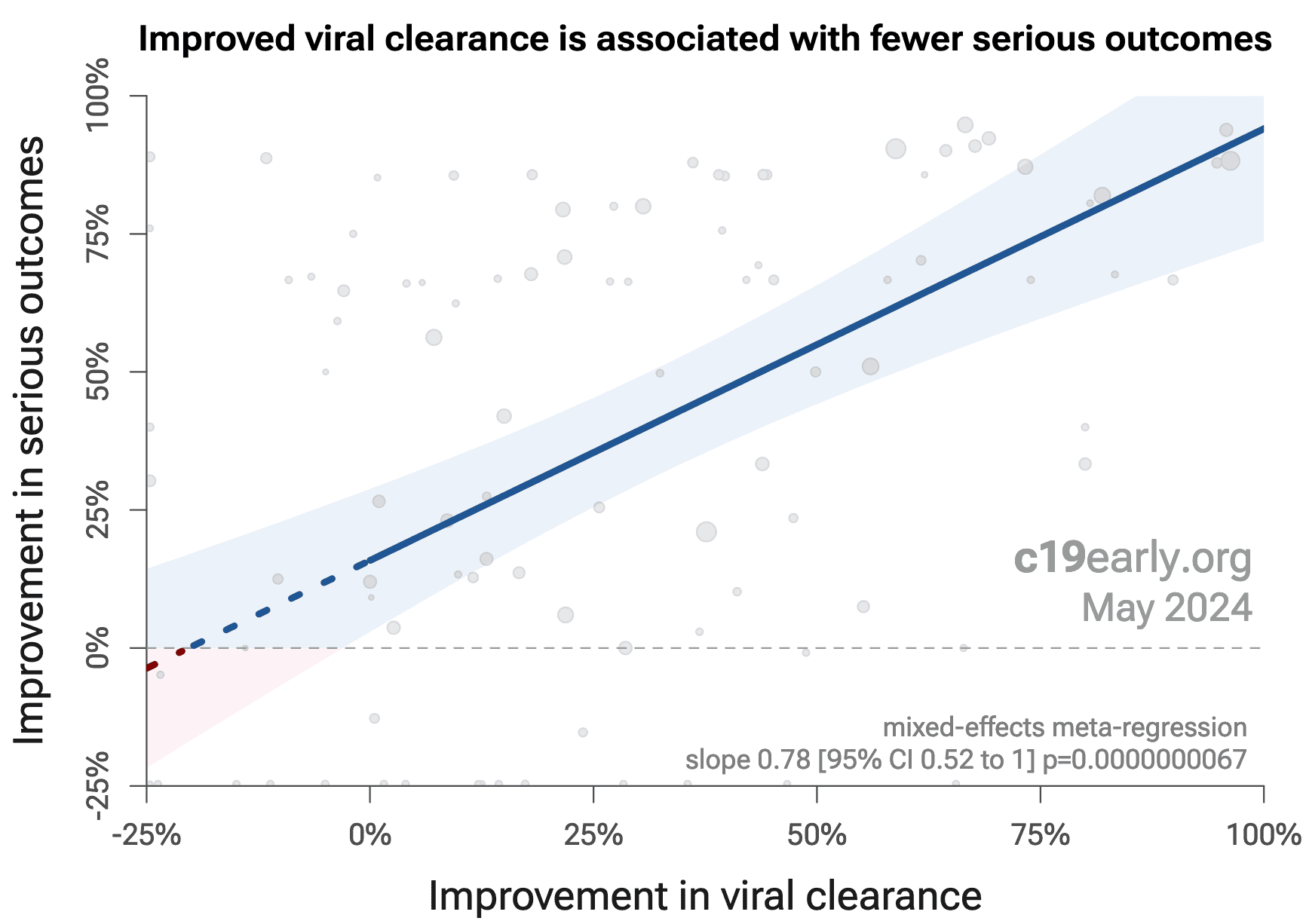
Figure 9 shows that improved viral clearance is strongly associated
with fewer serious outcomes. The association is very similar to
Singh et al., with higher confidence due to the larger number of
studies. As with Singh et al., the confidence increases
when excluding the outlier treatment, from p = 0.0000031 to p = 0.0000000067.
{kind=link}
Loading..
Figure 7. Lower hospitalization is associated with lower mortality, supporting pooled outcome analysis.
{kind=link}
Loading..
Figure 8. Improved recovery is associated with lower mortality, supporting pooled outcome analysis.
{kind=link}
Loading..
Figure 7. Improved viral clearance is associated with fewer serious outcomes, supporting pooled outcome analysis.
Currently, 44 of the treatments we analyze show statistically significant efficacy or harm, defined as ≥10% decreased risk or >0% increased risk from ≥3 studies. 88% of these have been confirmed with one or more specific outcomes, with a mean delay of 4.7 months. When restricting to RCTs only, 54% of treatments showing statistically significant efficacy/harm with pooled effects have been confirmed with one or more specific outcomes, with a mean delay of 5.5 months.
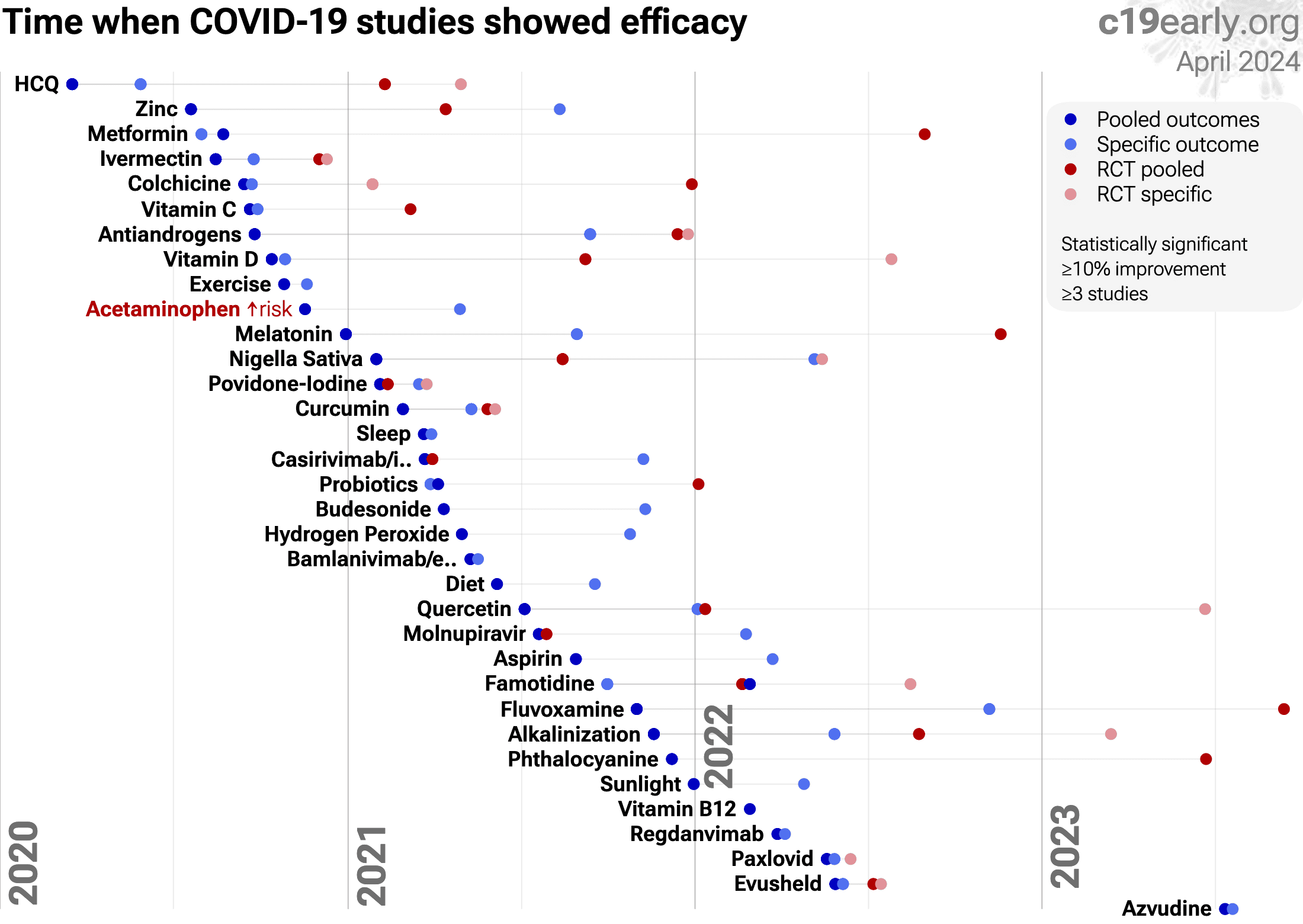
Figure 10 shows when treatments were found effective during the
pandemic. Pooled outcomes often resulted in earlier detection of efficacy.
{kind=link}
Loading..
Loading..
Figure 10. The time when studies showed that
treatments were effective, defined as statistically significant improvement of
≥10% from ≥3 studies.
Pooled results typically show efficacy earlier than specific
outcome results. Results from all studies often shows efficacy much earlier
than when restricting to RCTs.
Results reflect conditions as used in trials to date, these depend on the
population treated, treatment delay, and treatment regimen.
Pooled analysis could hide efficacy, for example a treatment that is
beneficial for late stage patients but has no effect on viral clearance may
show no efficacy if most studies only examine viral clearance. In practice, it
is rare for a non-antiviral treatment to report viral clearance and to not
report clinical outcomes; and in practice other sources of heterogeneity such
as difference in treatment delay is more likely to hide efficacy.
Analysis validates the use of pooled effects and shows significantly faster
detection of efficacy on average.
However, as with all meta analyses, it is important to review the different
studies included. We also present individual outcome analyses, which may be
more informative for specific use cases.
Larenas-Linnemann et al. present a review covering sleep for COVID-19.
SARS-CoV-2 infection and replication involves a complex interplay of 50+ host
and viral proteins and other factors Lui, Lv, Malone, Murigneux, Niarakis,
providing many therapeutic targets.
Over 7,000 compounds have been predicted to reduce COVID-19
risk c19early.org, either by directly
minimizing infection or replication, by supporting immune system function, or
by minimizing secondary complications.
Sleep can improve the absorption, metabolism, and utilization of nutrients, reduce chronic inflammation, improve cardiovascular health, improve comorbidities, and reduce stress. Sleep is crucial for the proper functioning of the immune system. During sleep, the body produces and releases cytokines and T cells that help fight infections, reduce inflammation, and create immune memory.
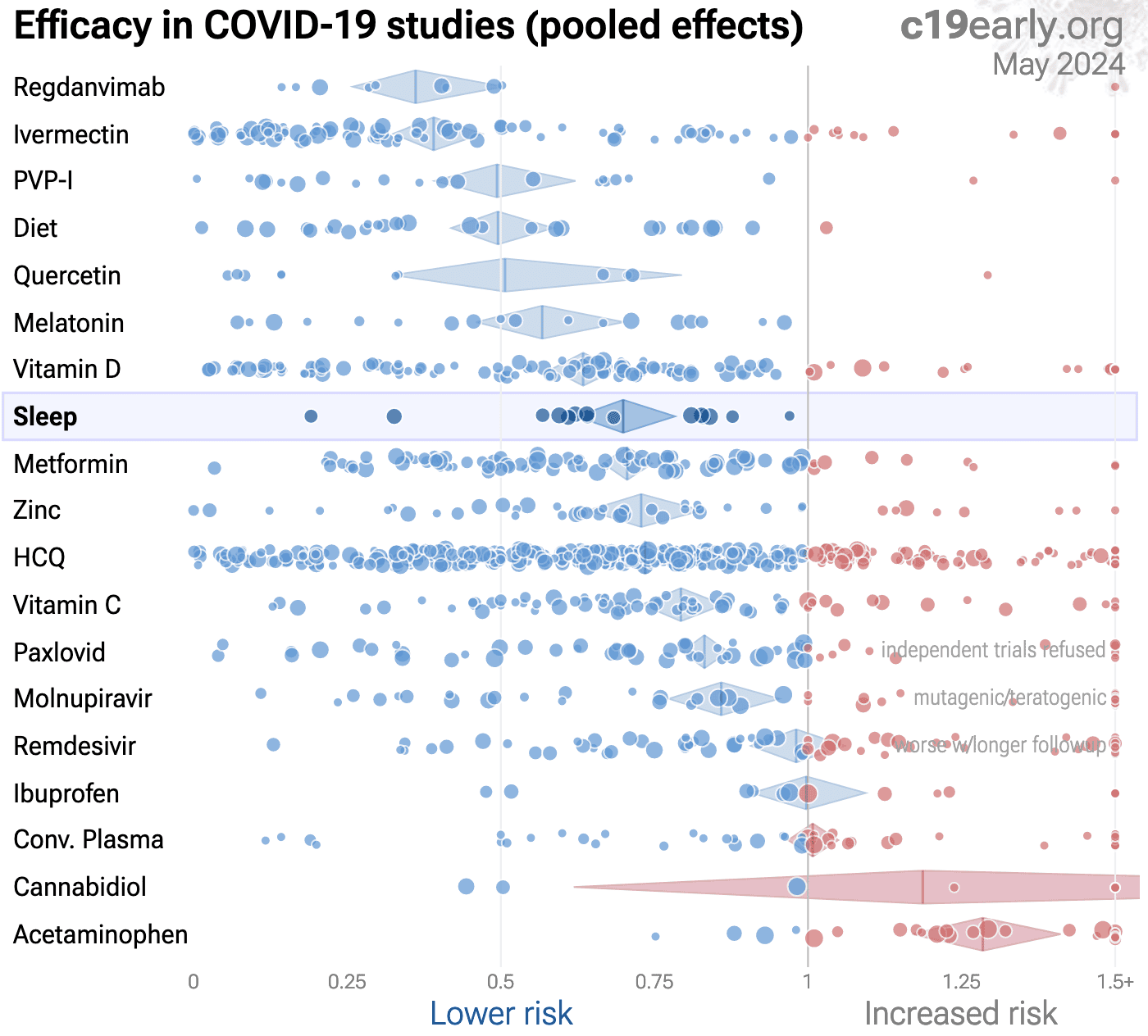
Figure 11 shows an overview of the results for sleep
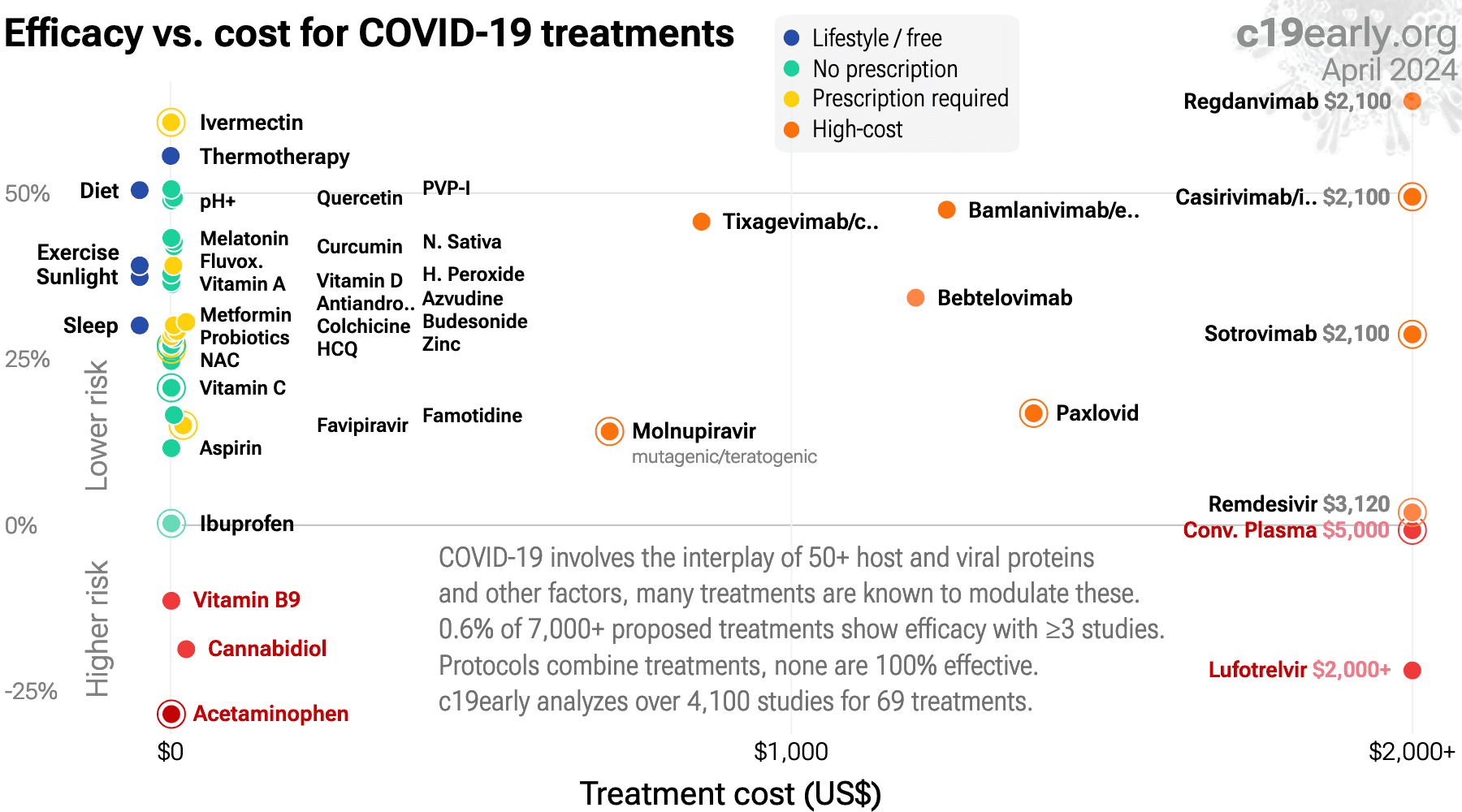
in the context of multiple COVID-19 treatments, and Figure 12 shows a plot
of efficacy vs. cost for COVID-19 treatments.
{kind=link}
Loading..
Figure 11.
Scatter plot showing results within the context of multiple COVID-19 treatments.
Diamonds shows the results of random effects meta-analysis.
0.6% of 7,000+ proposed treatments show efficacy
c19early.org (B).
{kind=link}
Loading..
Loading..
Figure 12. Efficacy vs. cost for COVID-19 treatments.
Sleep can improve the absorption, metabolism, and utilization of nutrients, reduce chronic inflammation, improve cardiovascular health, improve comorbidities, and reduce stress. Sleep is crucial for the proper functioning of the immune system. During sleep, the body produces and releases cytokines and T cells that help fight infections, reduce inflammation, and create immune memory.
Better sleep reduces risk for COVID-19.
Statistically significant lower risk is seen for mortality, hospitalization, and cases. 12 studies from 12 independent teams in 5 countries show statistically significant
improvements.
Meta analysis using the most serious outcome reported shows
30% [22‑38%] lower risk. Results are similar for peer-reviewed studies.
Results are robust — in exclusion sensitivity analysis 13 of 15
studies must be excluded to avoid finding statistically significant efficacy
in pooled analysis.
Studies analyze sleep quality before infection, and use different definitions of sleep quality.
{kind=link}
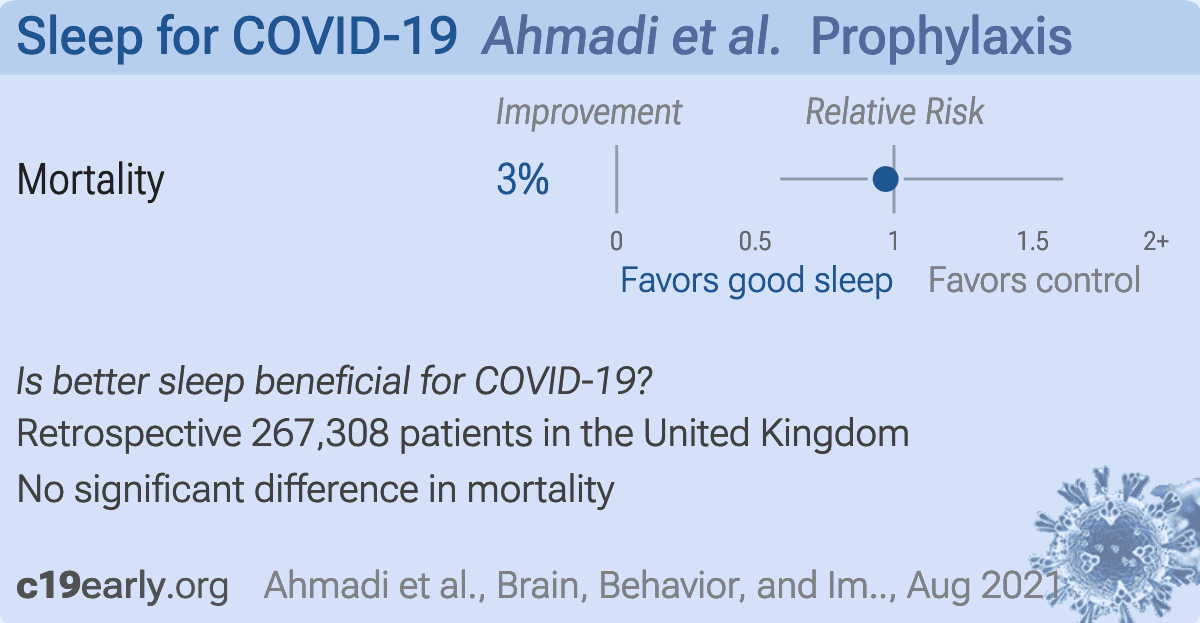
Ahmadi:
Retrospective 468,569 adults in the UK, showing no significant difference in COVID-19 mortality based on sleep quality.
{kind=link}
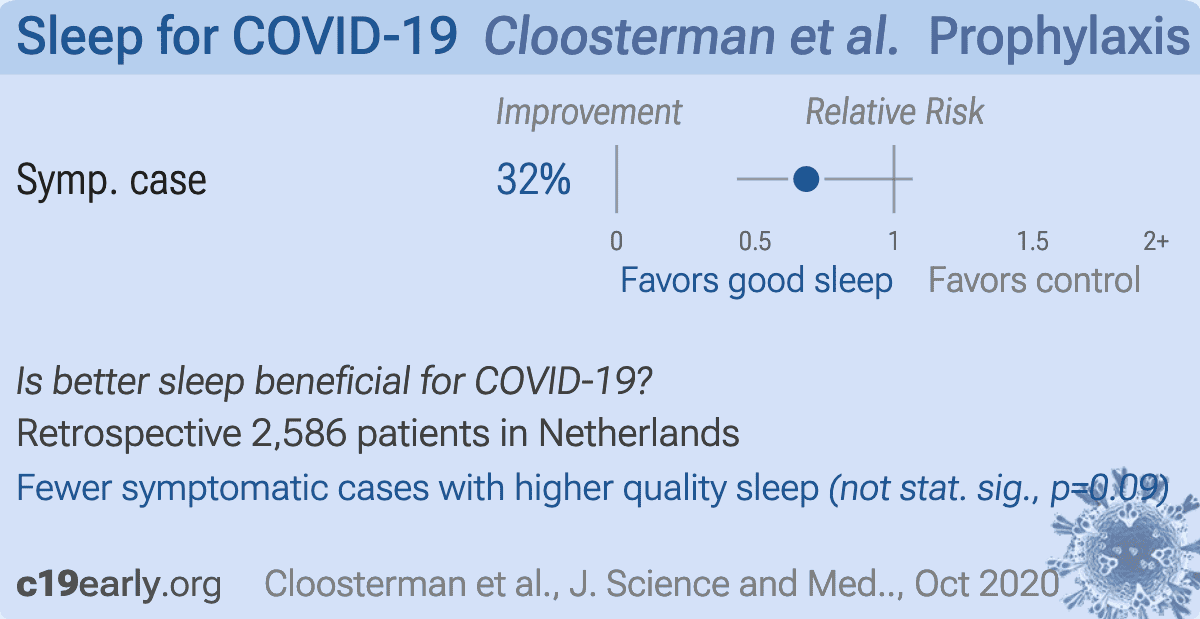
Cloosterman:
Analysis of 2,586 participants of a running injury prevention RCT in the Netherlands, showing higher risk of COVID-19 symptoms with sleep disturbance.
{kind=link}
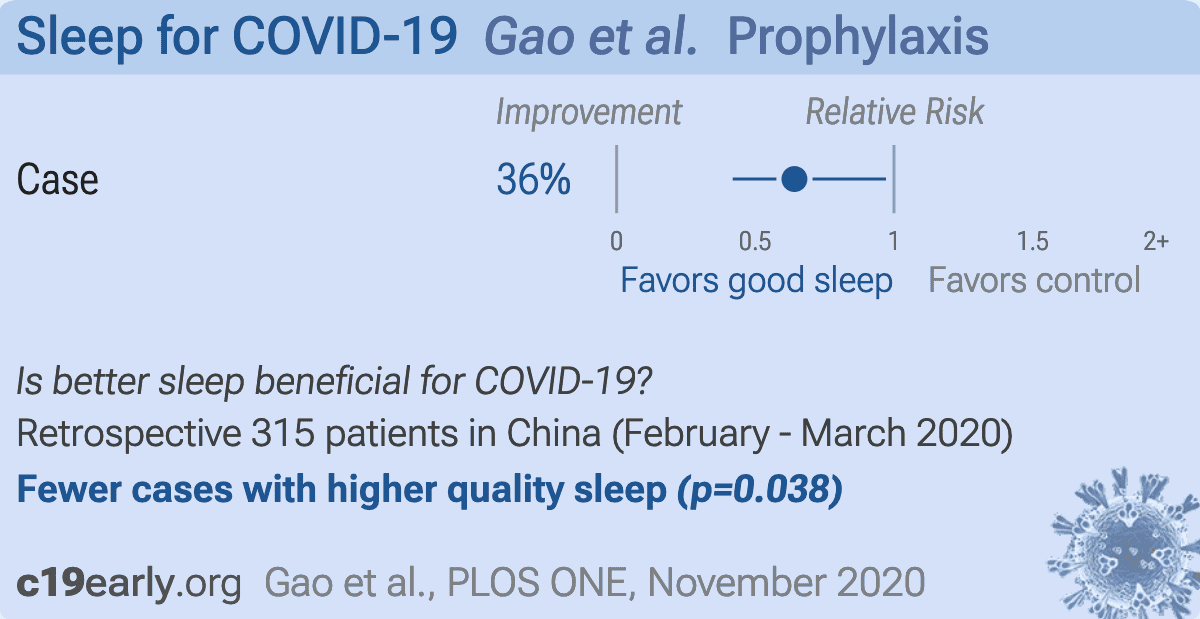
Gao:
Case control study in China with 105 cases and 210 matched controls, showing COVID-19 cases associated with lack of sleep.
{kind=link}
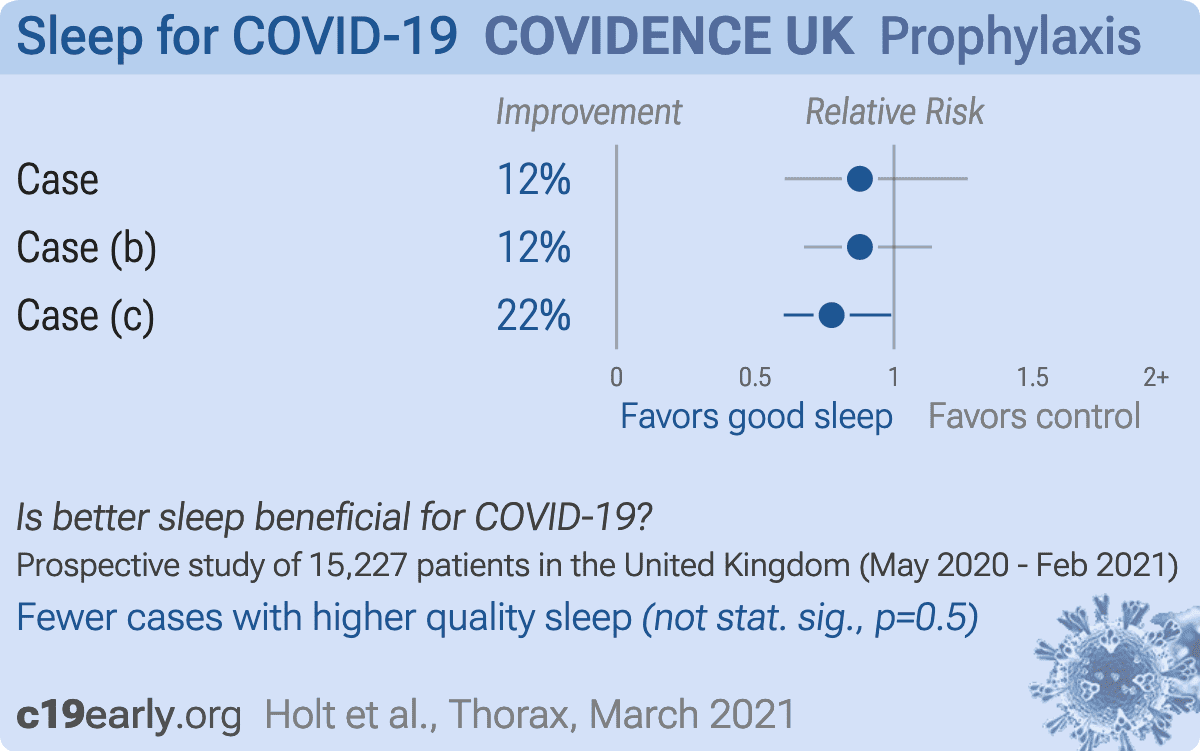
Holt:
Prospective survey-based study with 15,227 people in the UK, showing reduced risk of COVID-19 cases with 8 hours sleep, with statistical significance when compared with ≥9 hours. NCT04330599. COVIDENCE UK.
{kind=link}
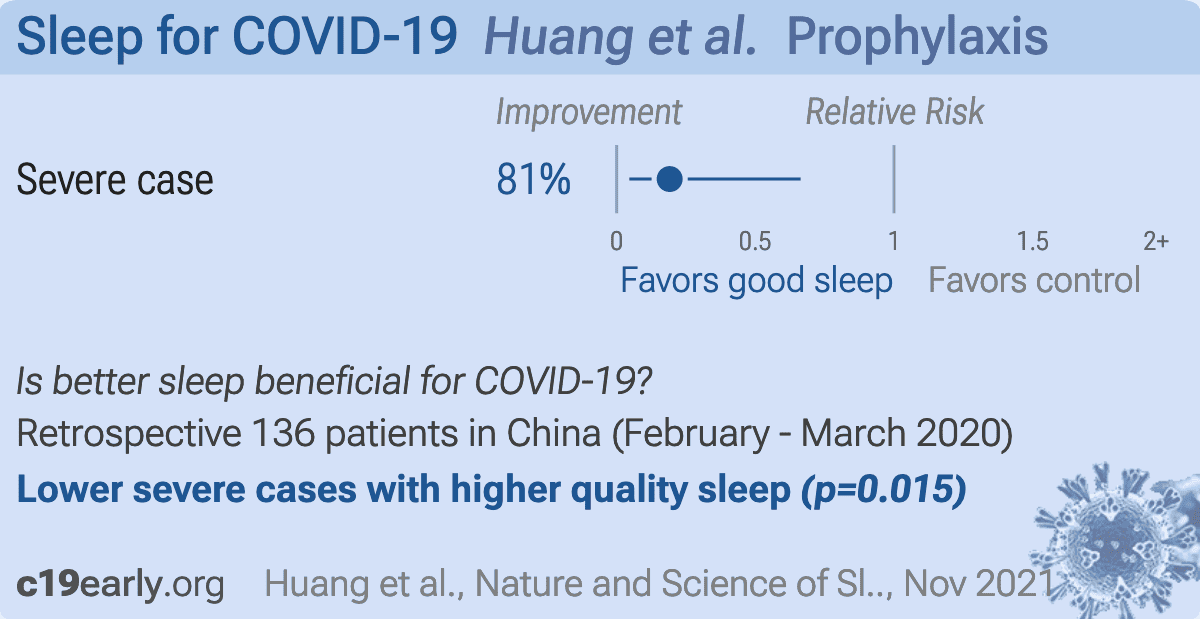
Huang:
Retrospective 164 COVID-19 patients and 188 controls in China, showing the risk of severe cases associated with lack of sleep.
{kind=link}
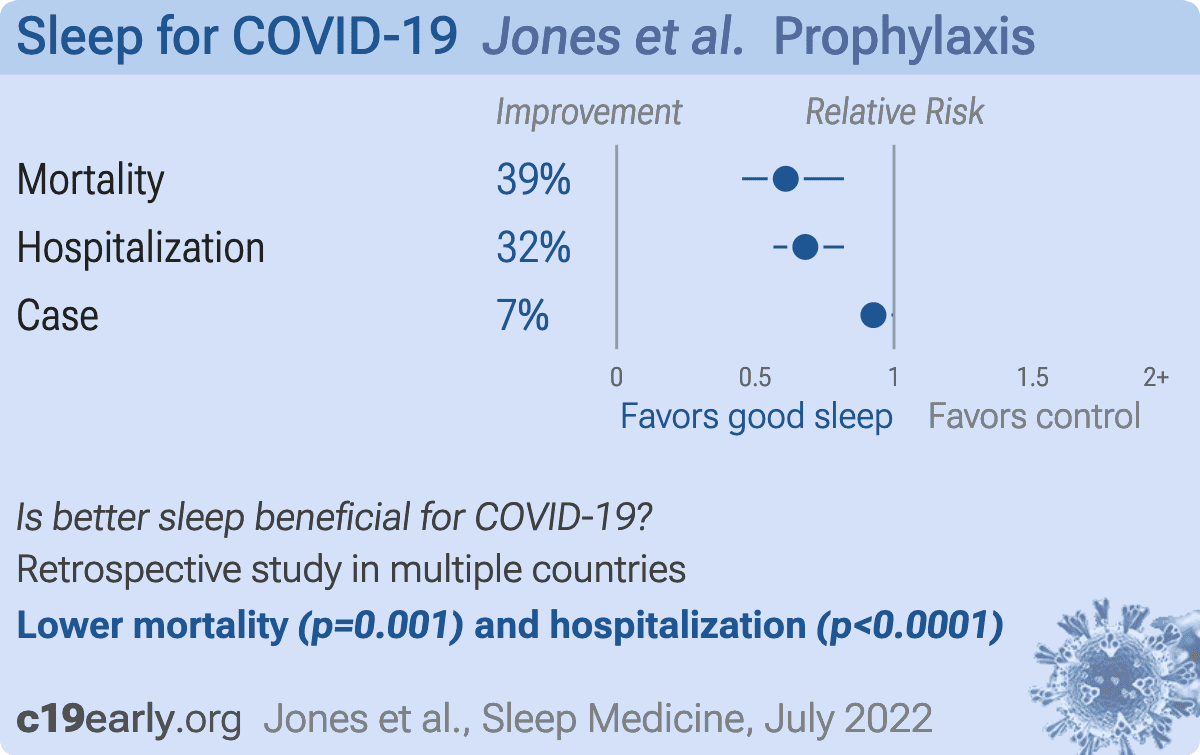
Jones:
FinnGen Mendelian randomization study showing higher risk of COVID-19 mortality, hospitalization, and infection with insomnia.
{kind=link}
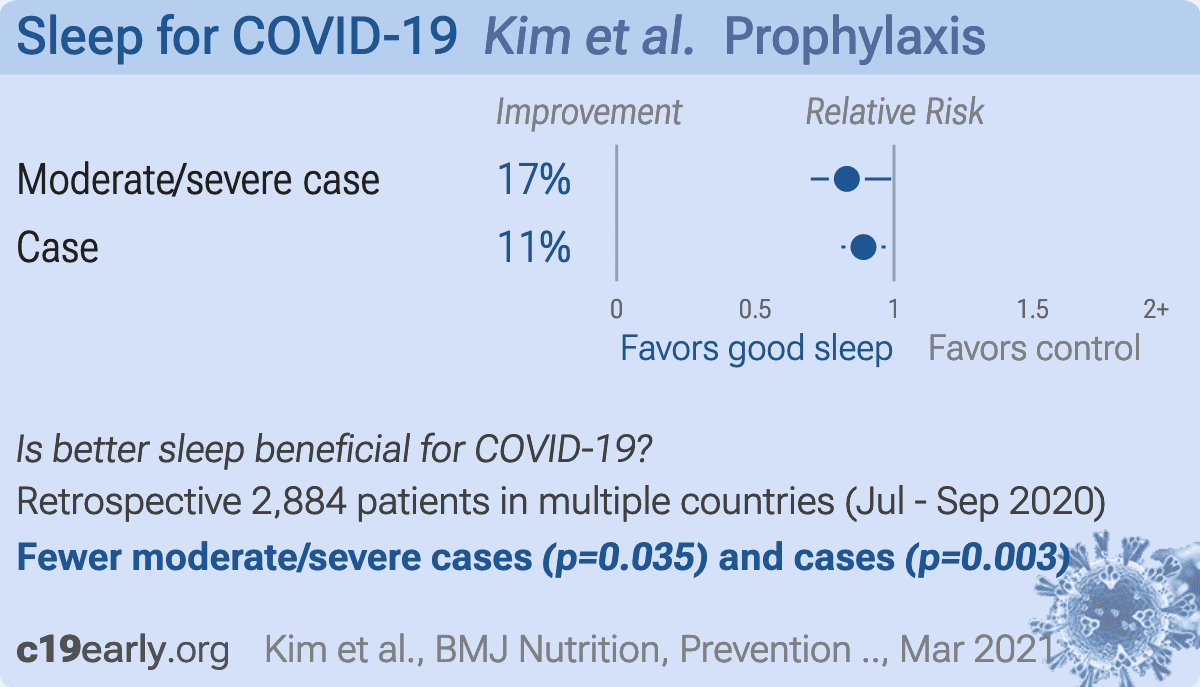
Kim:
Retrospective 2,884 high-risk healthcare workers in France, Germany, Italy, Spain, UK, and the USA, showing shorter sleep duration associated with increased risk of COVID-19 cases and severity.
{kind=link}
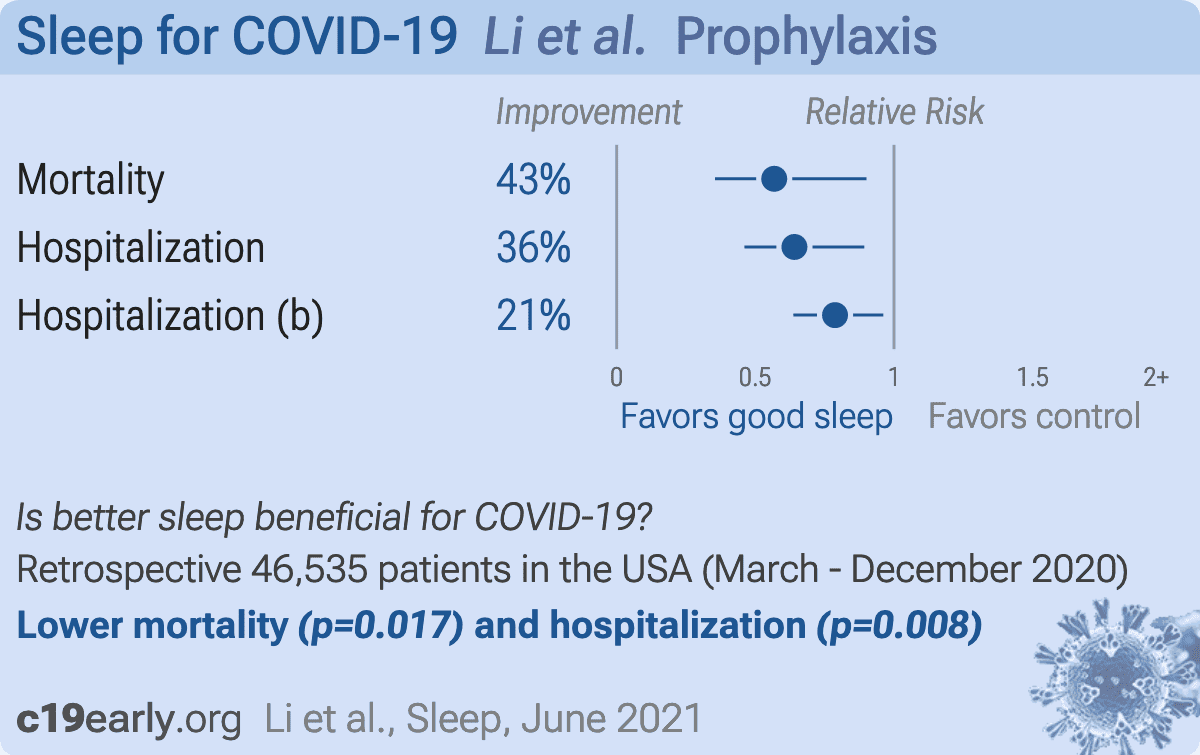
Li:
UK Biobank retrospective, 46,535 participants with sleep behavior assessed between 2006 and 2010, showing higher risk of hospitalization and mortality with poor sleep.
{kind=link}
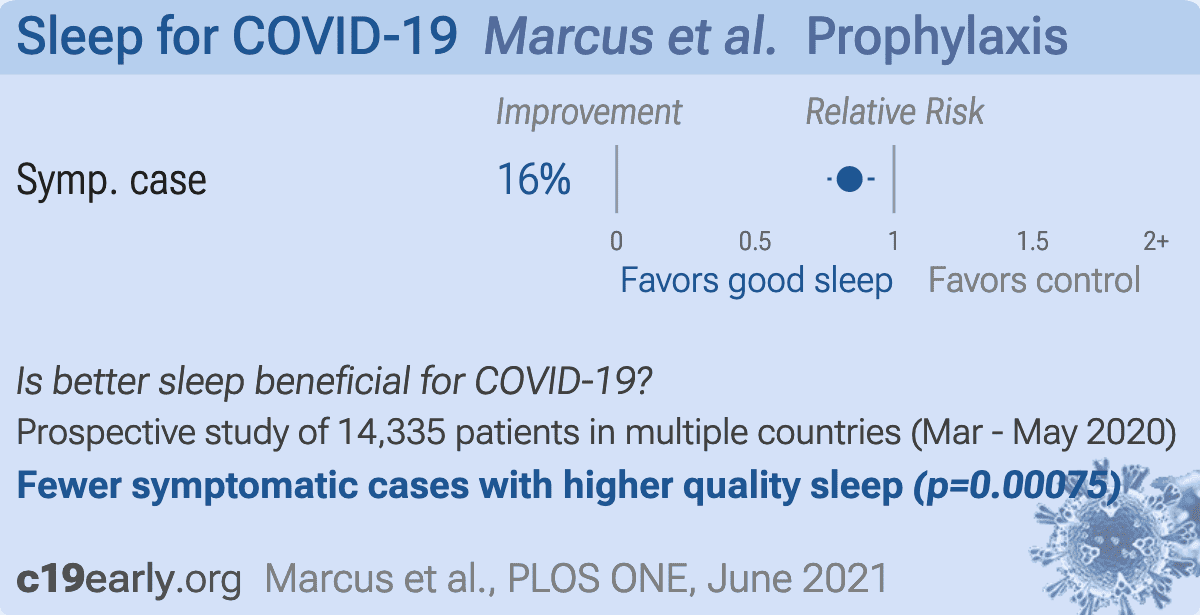
Marcus:
Prospective survey based study with 14,335 participants, showing risk of viral symptoms associated with shorter sleep duration.
{kind=link}
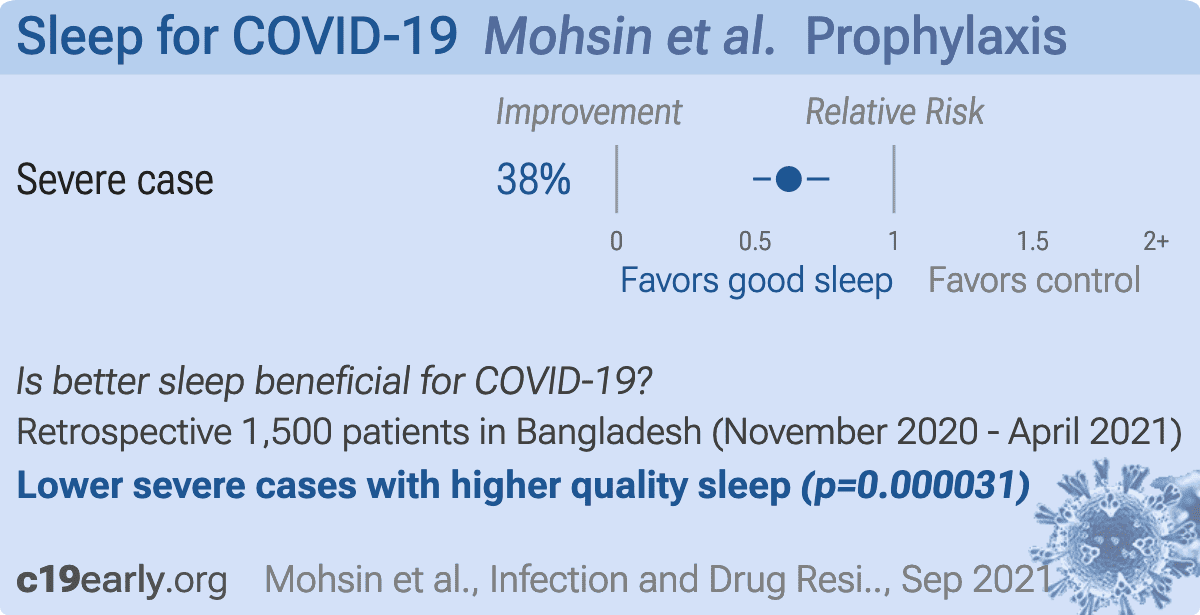
Mohsin:
Retrospective 1,500 COVID+ patients in Bangladesh, showing lower risk of severe cases with good sleep.
{kind=link}
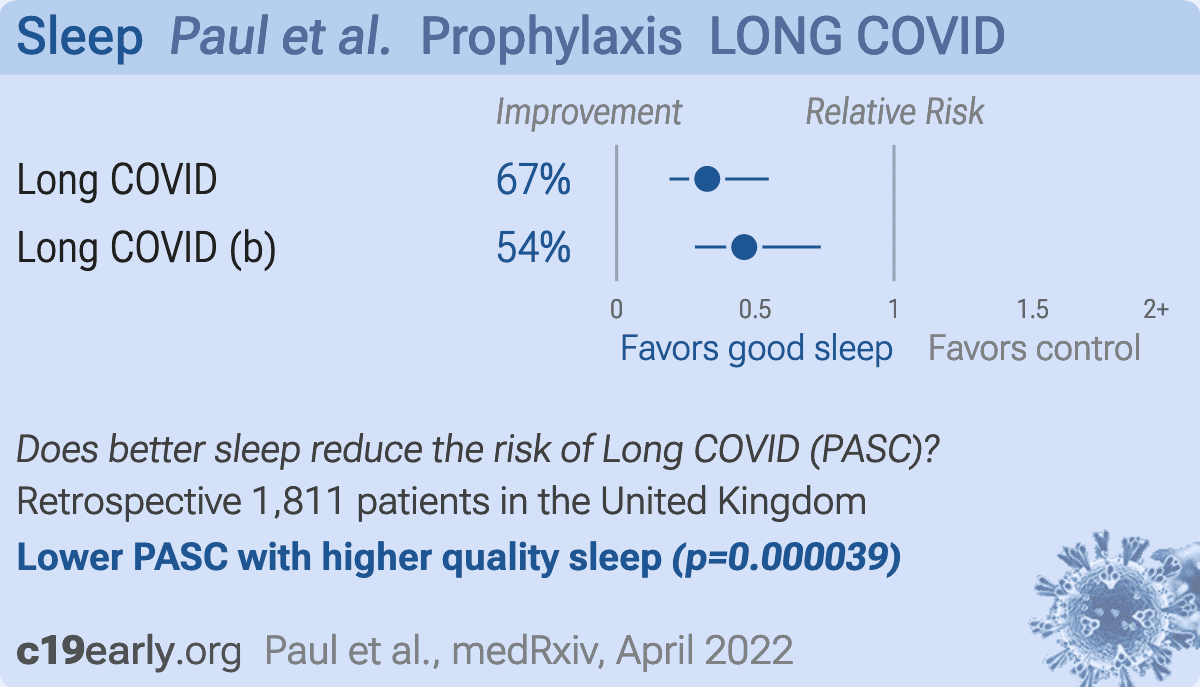
Paul:
Retrospective 1,811 COVID-19 patients in the UK, showing lower risk of self-reported long COVID with good sleep quality in the month before infection.
{kind=link}
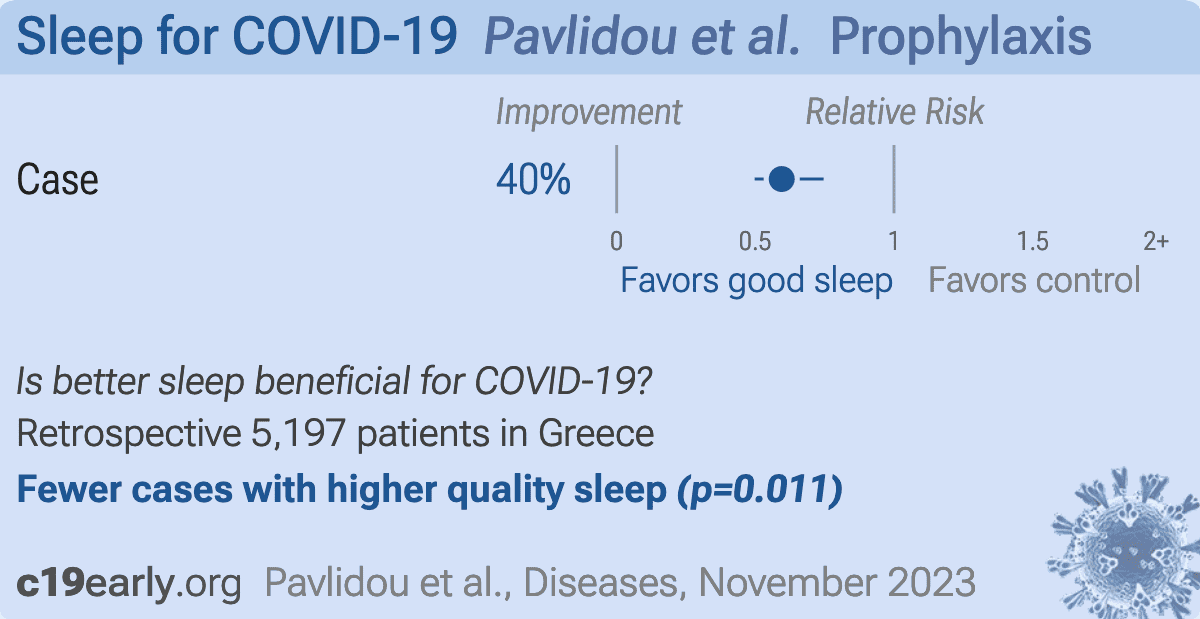
Pavlidou:
Retrospective 5,197 Greek adults over 65. After adjustment for confounders, COVID-19 infection was independently associated with poor sleep, low physical activity, low Mediterranean diet adherence, living in urban areas, smoking, obesity, depression, anxiety, stress, and poor health-related quality of life.
{kind=link}
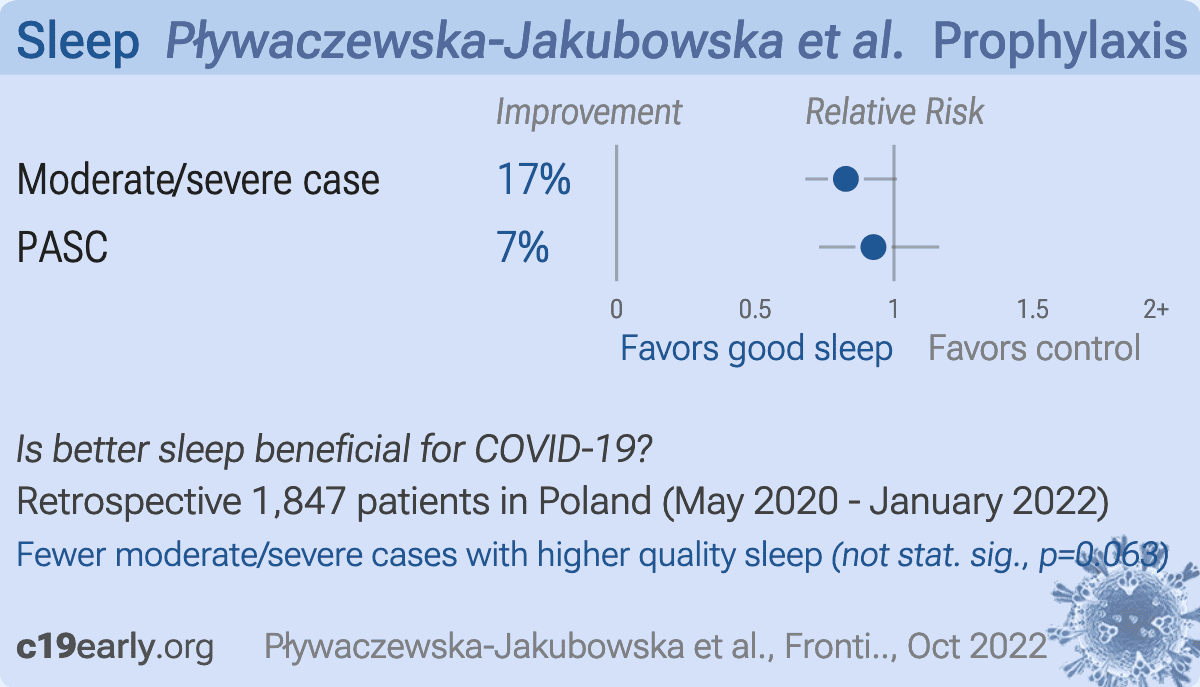
Pływaczewska-Jakubowska:
Retrospective 1,847 COVID+ patients in Poland, showing lower moderate/severe cases with improved sleep, without statistical significance. Hospitalized patients were excluded.
{kind=link}
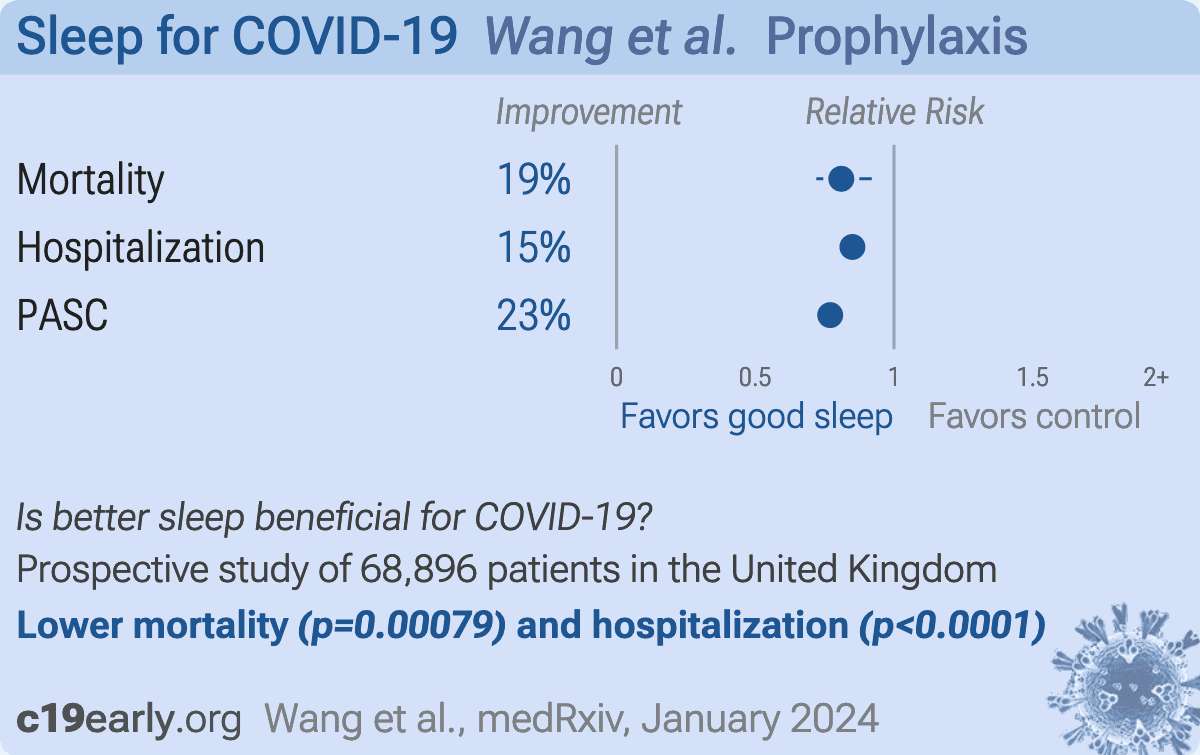
Wang:
Prospective study of 68,896 UK Biobank participants with COVID-19 showing adherence to a healthy lifestyle prior to infection, characterized by 10 factors including adequate physical activity and sleep, not smoking, and a healthy BMI, was associated with a significantly lower risk of mortality, hospitalization, and post-COVID multisystem sequelae. Risk decreased monotonically for increasing numbers of healthy lifestyle factors from 5-10. Reduced risks were evident across cardiovascular, metabolic, neurologic, respiratory, and other disorders over 210 days following infection, during both acute and post-acute phases, regardless of age, sex, ethnicity, test setting, vaccination status, or SARS-CoV-2 variant.
{kind=link}
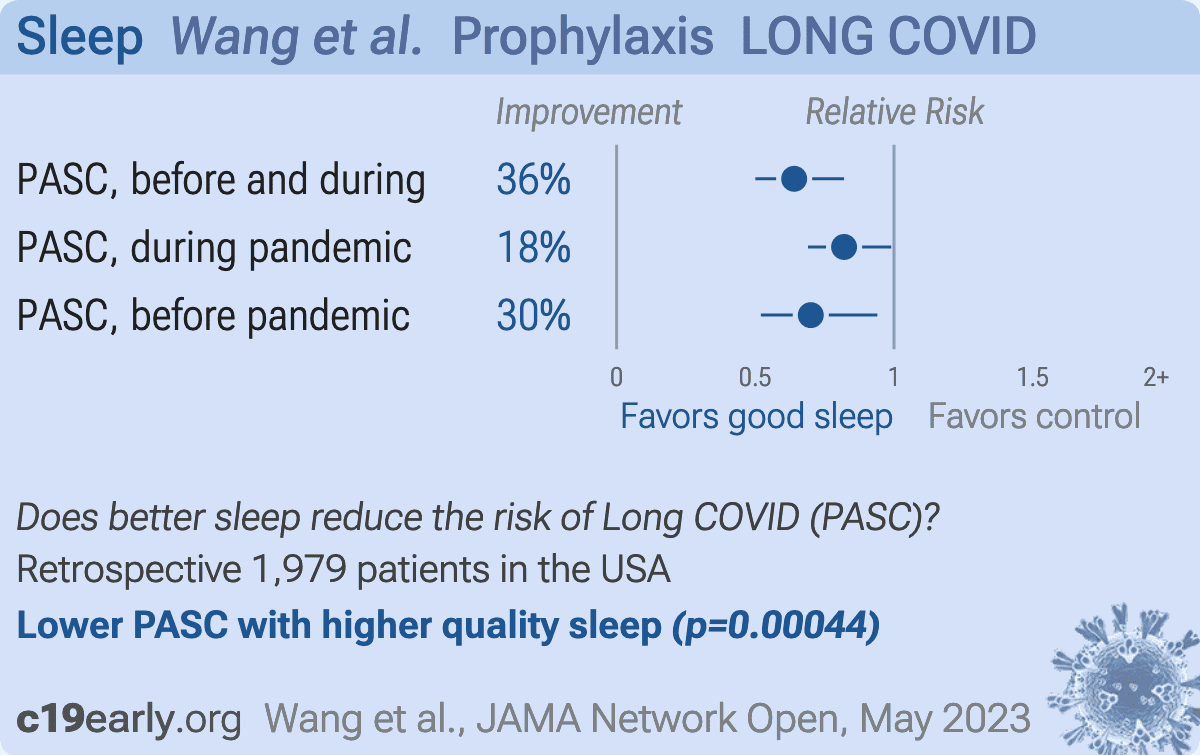
Wang (B):
Retrospective 1,979 nurses in the USA, showing lower risk of long COVID with better sleep quality.
We perform ongoing searches of PubMed, medRxiv, Europe PMC,
ClinicalTrials.gov, The Cochrane Library, Google Scholar, Research
Square, ScienceDirect, Oxford University Press, the reference lists of other
studies and meta-analyses, and submissions to the site c19early.org.
Search terms are sleep AND COVID-19. Automated searches are performed twice daily, with all matches reviewed for inclusion.
All studies regarding the use of sleep for COVID-19 that report
a comparison with a control group are included in the main analysis.
This is a living analysis and is updated regularly.
We extracted effect sizes and associated data from all studies.
If studies report multiple kinds of effects then the most serious
outcome is used in pooled analysis, while other outcomes are included in the
outcome specific analyses. For example, if effects for mortality and cases are
both reported, the effect for mortality is used, this may be different to the
effect that a study focused on.
If symptomatic
results are reported at multiple times, we used the latest time, for example
if mortality results are provided at 14 days and 28 days, the results at 28
days have preference. Mortality alone is preferred over combined outcomes.
Outcomes with zero events in both arms are not used, the next most serious
outcome with one or more events is used. For example, in low-risk populations
with no mortality, a reduction in mortality with treatment is not possible,
however a reduction in hospitalization, for example, is still valuable.
Clinical outcomes are considered more important than viral test status. When
basically all patients recover in both treatment and control groups,
preference for viral clearance and recovery is given to results mid-recovery
where available. After most or all patients have recovered there is little or
no room for an effective treatment to do better, however faster recovery is
valuable.
If only individual symptom data is available, the most serious symptom has
priority, for example difficulty breathing or low SpO2 is more
important than cough.
When results provide an odds ratio, we compute the relative risk when
possible, or convert to a relative risk according to Zhang.
Reported confidence intervals and p-values were used when available,
using adjusted values when provided. If multiple types of adjustments are
reported propensity score matching and multivariable regression has preference
over propensity score matching or weighting, which has preference over
multivariable regression. Adjusted results have preference over unadjusted
results for a more serious outcome when the adjustments significantly alter
results. When needed, conversion between reported p-values and
confidence intervals followed Altman, Altman (B), and Fisher's exact
test was used to calculate p-values for event data. If continuity
correction for zero values is required, we use the reciprocal of the opposite
arm with the sum of the correction factors equal to 1 Sweeting.
Results are expressed with RR < 1.0 favoring treatment, and using the risk of
a negative outcome when applicable (for example, the risk of death rather than
the risk of survival). If studies only report relative continuous values such
as relative times, the ratio of the time for the treatment group versus the
time for the control group is used. Calculations are done in Python
(3.12.3) with
scipy (1.13.0), pythonmeta (1.26), numpy (1.26.4), statsmodels (0.14.2), and plotly (5.21.0).
Forest plots are computed using PythonMeta Deng
with the DerSimonian and Laird random effects model (the fixed effect
assumption is not plausible in this case) and inverse variance weighting.
Results are presented with 95% confidence intervals. Heterogeneity among studies was
assessed using the I2 statistic.
Mixed-effects meta-regression results are computed with R (4.1.2) using the metafor
(3.0-2) and rms (6.2-0) packages, and using the most serious sufficiently powered outcome.
For all statistical tests, a p-value less than 0.05 was considered statistically significant.
Grobid 0.8.0 is used to parse PDF documents.
We have classified studies as early treatment if most patients
are not already at a severe stage at the time of treatment (for example based
on oxygen status or lung involvement), and treatment started within 5 days of
the onset of symptoms. If studies contain a mix of early treatment and late
treatment patients, we consider the treatment time of patients contributing
most to the events (for example, consider a study where most patients are
treated early but late treatment patients are included, and all mortality
events were observed with late treatment patients).
We note that a shorter time may be preferable. Antivirals are typically only
considered effective when used within a shorter timeframe, for example 0-36 or
0-48 hours for oseltamivir, with longer delays not being effective
McLean, Treanor.
We received no funding, this research is done in our spare
time. We have no affiliations with any pharmaceutical companies or political
parties.
A summary of study results is below. Please submit
updates and corrections at https://c19early.org/slmeta.html.
Effect extraction follows pre-specified rules as detailed above
and gives priority to more serious outcomes.
For pooled analyses, the first (most serious) outcome is used, which may
differ from the effect a paper focuses on.
Other outcomes are used in outcome specific analyses.
| Ahmadi, 8/31/2021, retrospective, United Kingdom, peer-reviewed, 5 authors. | risk of death, 3.0% lower, RR 0.97, p = 0.91, adjusted per study, good vs. poor, model 2, multivariable. |
| Cloosterman, 10/21/2020, retrospective, Netherlands, peer-reviewed, 4 authors. | risk of symptomatic case, 31.6% lower, RR 0.68, p = 0.09, higher quality sleep 31 of 201 (15.4%), lower quality sleep 222 of 2,385 (9.3%), inverted to make RR<1 favor higher quality sleep, odds ratio converted to relative risk. |
| Gao, 11/5/2020, retrospective, China, peer-reviewed, survey, median age 55.0, 11 authors, study period 10 February, 2020 - 1 March, 2020. | risk of case, 35.9% lower, HR 0.64, p = 0.04, higher quality sleep 73 of 105 (69.5%) cases, 179 of 210 (85.2%) controls, NNT 4.6, inverted to make HR<1 favor higher quality sleep, case control OR, Cox proportional hazards. |
| Holt, 3/30/2021, prospective, United Kingdom, peer-reviewed, 34 authors, study period 1 May, 2020 - 5 February, 2021, trial NCT04330599 (history) (COVIDENCE UK). | risk of case, 12.3% lower, OR 0.88, p = 0.50, adjusted per study, inverted to make OR<1 favor higher quality sleep, fully adjusted, 8 hours vs. ≤6 hours, RR approximated with OR. |
| risk of case, 12.3% lower, OR 0.88, p = 0.33, adjusted per study, inverted to make OR<1 favor higher quality sleep, fully adjusted, 8 hours vs. 7 hours, RR approximated with OR. | |
| risk of case, 22.5% lower, OR 0.78, p = 0.04, adjusted per study, inverted to make OR<1 favor higher quality sleep, fully adjusted, 8 hours vs. ≥9 hours, RR approximated with OR. | |
| Huang, 11/30/2021, retrospective, China, peer-reviewed, survey, 5 authors, study period 10 February, 2020 - 28 March, 2020. | risk of severe case, 80.9% lower, RR 0.19, p = 0.02, higher quality sleep 12 of 127 (9.4%), lower quality sleep 4 of 9 (44.4%), NNT 2.9, adjusted per study, inverted to make RR<1 favor higher quality sleep, odds ratio converted to relative risk, recommended vs. lack of sleep, multivariable. |
| Jones, 7/21/2022, retrospective, multiple countries, peer-reviewed, 12 authors. | risk of death, 39.0% lower, OR 0.61, p = 0.001, inverted to make OR<1 favor higher quality sleep, RR approximated with OR. |
| risk of hospitalization, 32.0% lower, OR 0.68, p < 0.001, inverted to make OR<1 favor higher quality sleep, RR approximated with OR. | |
| risk of case, 7.4% lower, OR 0.93, p = 0.04, inverted to make OR<1 favor higher quality sleep, RR approximated with OR. | |
| Kim, 3/22/2021, retrospective, multiple countries, peer-reviewed, survey, mean age 48.0, 8 authors, study period 17 July, 2020 - 25 September, 2020. | risk of moderate/severe case, 17.0% lower, OR 0.83, p = 0.03, per extra hour of sleep, RR approximated with OR. |
| risk of case, 11.0% lower, OR 0.89, p = 0.003, per extra hour of sleep, model 3, RR approximated with OR. | |
| Li, 6/18/2021, retrospective, USA, peer-reviewed, mean age 69.4, 8 authors, study period March 2020 - December 2020. | risk of death, 43.2% lower, OR 0.57, p = 0.02, inverted to make OR<1 favor higher quality sleep, fully adjusted model C, significant poor sleep burden, RR approximated with OR. |
| risk of hospitalization, 35.9% lower, OR 0.64, p = 0.008, inverted to make OR<1 favor higher quality sleep, fully adjusted model C, significant poor sleep burden, RR approximated with OR. | |
| risk of hospitalization, 21.3% lower, OR 0.79, p = 0.02, inverted to make OR<1 favor higher quality sleep, fully adjusted model C, moderate poor sleep burden, RR approximated with OR. | |
| Marcus, 6/17/2021, prospective, multiple countries, peer-reviewed, survey, 12 authors, study period 26 March, 2020 - 3 May, 2020. | risk of symptomatic case, 16.0% lower, OR 0.84, p < 0.001, adjusted per study, per extra hour sleep, multivariable, RR approximated with OR. |
| Mohsin, 9/30/2021, retrospective, Bangladesh, peer-reviewed, survey, 10 authors, study period November 2020 - April 2021. | risk of severe case, 37.9% lower, RR 0.62, p < 0.001, higher quality sleep 327 of 948 (34.5%), lower quality sleep 273 of 552 (49.5%), NNT 6.7, adjusted per study, inverted to make RR<1 favor higher quality sleep, odds ratio converted to relative risk, sleep disturbance, multivariable. |
| Paul, 4/13/2022, retrospective, United Kingdom, preprint, survey, 2 authors. | risk of long COVID, 67.3% lower, RR 0.33, p < 0.001, adjusted per study, inverted to make RR<1 favor higher quality sleep, odds ratio converted to relative risk, very good/good vs. not good/very poor, multivariable, model 4, control prevalance approximated with overall prevalence. |
| risk of long COVID, 54.0% lower, RR 0.46, p = 0.002, adjusted per study, inverted to make RR<1 favor higher quality sleep, odds ratio converted to relative risk, very good/good vs. average, multivariable, model 4, control prevalance approximated with overall prevalence. | |
| Pavlidou, 11/9/2023, retrospective, Greece, peer-reviewed, 14 authors. | risk of case, 40.5% lower, OR 0.60, p = 0.01, higher quality sleep 3,345, lower quality sleep 1,852, adjusted per study, inverted to make OR<1 favor higher quality sleep, adequate vs. inadequate sleep, multivariable, RR approximated with OR. |
| Pływaczewska-Jakubowska, 10/24/2022, retrospective, Poland, peer-reviewed, median age 51.0, 5 authors, study period May 2020 - January 2022. | risk of moderate/severe case, 17.4% lower, OR 0.83, p = 0.06, higher quality sleep 1,225, lower quality sleep 622, adjusted per study, inverted to make OR<1 favor higher quality sleep, higher quality sleep vs. insomnia or falling asleep after midnight or nightshifts, multivariable, model 3, RR approximated with OR. |
| risk of PASC, 7.4% lower, OR 0.93, p = 0.51, higher quality sleep 1,015, lower quality sleep 502, adjusted per study, inverted to make OR<1 favor higher quality sleep, higher quality sleep vs. insomnia or falling asleep after midnight or nightshifts, multivariable, model 3, RR approximated with OR. | |
| Wang, 1/31/2024, prospective, United Kingdom, preprint, 10 authors. | risk of death, 19.0% lower, HR 0.81, p < 0.001, higher quality sleep 50,777, lower quality sleep 18,119, adjusted per study, 7-9 hrs vs. <7 or >9, multivariable. |
| risk of hospitalization, 15.0% lower, HR 0.85, p < 0.001, higher quality sleep 50,777, lower quality sleep 18,119, adjusted per study, 7-9 hrs vs. <7 or >9, multivariable. | |
| risk of PASC, 23.0% lower, HR 0.77, p < 0.001, higher quality sleep 50,777, lower quality sleep 18,119, adjusted per study, 7-9 hrs vs. <7 or >9, multivariable. | |
| Wang (B), 5/30/2023, retrospective, USA, peer-reviewed, 6 authors. | risk of PASC, 36.0% lower, RR 0.64, p < 0.001, higher quality sleep 559, lower quality sleep 180, adjusted per study, healthy sleep before and during the pandemic, multivariable. |
| risk of PASC, 18.0% lower, RR 0.82, p = 0.03, adjusted per study, healthy sleep during the pandemic, multivariable. | |
| risk of PASC, 30.0% lower, RR 0.70, p = 0.02, higher quality sleep 238, lower quality sleep 166, adjusted per study, healthy sleep before the pandemic, sleep score 5 vs. score 0 or 1, multivariable. |
Ahmadi et al., Lifestyle risk factors and infectious disease mortality, including COVID-19, among middle aged and older adults: Evidence from a community-based cohort study in the United Kingdom, Brain, Behavior, and Immunity, doi:10.1016/j.bbi.2021.04.022.
Altman (B) et al., How to obtain the confidence interval from a P value, BMJ, doi:10.1136/bmj.d2090.
Cloosterman et al., Running behavior and symptoms of respiratory tract infection during the COVID-19 pandemic, Journal of Science and Medicine in Sport, doi:10.1016/j.jsams.2020.10.009.
Davidson et al., No evidence of important difference in summary treatment effects between COVID-19 preprints and peer-reviewed publications: a meta-epidemiological study, Journal of Clinical Epidemiology, doi:10.1016/j.jclinepi.2023.08.011.
Gao et al., The impact of individual lifestyle and status on the acquisition of COVID-19: A case—Control study, PLOS ONE, doi:10.1371/journal.pone.0241540.
Holt et al., Risk factors for developing COVID-19: a population-based longitudinal study (COVIDENCE UK), Thorax, doi:10.1136/thoraxjnl-2021-217487.
Huang et al., Reduced Sleep in the Week Prior to Diagnosis of COVID-19 is Associated with the Severity of COVID-19, Nature and Science of Sleep, doi:10.2147/NSS.S263488.
Jones et al., Public health impact of poor sleep on COVID-19, influenza and upper respiratory infections, Sleep Medicine, doi:10.1016/j.sleep.2022.05.369.
Kim et al., COVID-19 illness in relation to sleep and burnout, BMJ Nutrition, Prevention & Health, doi:10.1136/bmjnph-2021-000228.
Larenas-Linnemann et al., Enhancing innate immunity against virus in times of COVID-19: Trying to untangle facts from fictions, World Allergy Organization Journal, doi:10.1016/j.waojou.2020.100476.
Li et al., Poor sleep behavior burden and risk of COVID-19 mortality and hospitalization, Sleep, doi:10.1093/sleep/zsab138.
Lui et al., Nsp1 facilitates SARS-CoV-2 replication through calcineurin-NFAT signaling, Virology, doi:10.1128/mbio.00392-24.
Lv et al., Host proviral and antiviral factors for SARS-CoV-2, Virus Genes, doi:10.1007/s11262-021-01869-2.
Malone et al., Structures and functions of coronavirus replication–transcription complexes and their relevance for SARS-CoV-2 drug design, Nature Reviews Molecular Cell Biology, doi:10.1038/s41580-021-00432-z.
Marcus et al., Predictors of incident viral symptoms ascertained in the era of COVID-19, PLOS ONE, doi:10.1371/journal.pone.0253120.
McLean et al., Impact of Late Oseltamivir Treatment on Influenza Symptoms in the Outpatient Setting: Results of a Randomized Trial, Open Forum Infect. Dis. September 2015, 2:3, doi:10.1093/ofid/ofv100.
Mohsin et al., Lifestyle and Comorbidity-Related Risk Factors of Severe and Critical COVID-19 Infection: A Comparative Study Among Survived COVID-19 Patients in Bangladesh, Infection and Drug Resistance, doi:10.2147/IDR.S331470.
Murigneux et al., Proteomic analysis of SARS-CoV-2 particles unveils a key role of G3BP proteins in viral assembly, Nature Communications, doi:10.1038/s41467-024-44958-0.
Niarakis et al., Drug-target identification in COVID-19 disease mechanisms using computational systems biology approaches, Frontiers in Immunology, doi:10.3389/fimmu.2023.1282859.
Paul et al., Health behaviours the month prior to COVID-19 infection and the development of self-reported long COVID and specific long COVID symptoms: A longitudinal analysis of 1,811 UK adults, medRxiv, doi:10.1101/2022.04.12.22273792.
Pavlidou et al., Association of COVID-19 Infection with Sociodemographic, Anthropometric and Lifestyle Factors: A Cross-Sectional Study in an Older Adults’ Population Aged over 65 Years Old, Diseases, doi:10.3390/diseases11040165.
Pływaczewska-Jakubowska et al., Lifestyle, course of COVID-19, and risk of Long-COVID in non-hospitalized patients, Frontiers in Medicine, doi:10.3389/fmed.2022.1036556.
Singh et al., The relationship between viral clearance rates and disease progression in early symptomatic COVID-19: a systematic review and meta-regression analysis, Journal of Antimicrobial Chemotherapy, doi:10.1093/jac/dkae045.
Sweeting et al., What to add to nothing? Use and avoidance of continuity corrections in meta-analysis of sparse data, Statistics in Medicine, doi:10.1002/sim.1761.
Treanor et al., Efficacy and Safety of the Oral Neuraminidase Inhibitor Oseltamivir in Treating Acute Influenza: A Randomized Controlled Trial, JAMA, 2000, 283:8, 1016-1024, doi:10.1001/jama.283.8.1016.
Wang et al., Healthy lifestyle for the prevention of post-COVID-19 multisystem sequelae, hospitalization, and death: a prospective cohort study, medRxiv, doi:10.1101/2024.01.30.24302040.
Wang (B) et al., Multidimensional Sleep Health Prior to SARS-CoV-2 Infection and Risk of Post–COVID-19 Condition, JAMA Network Open, doi:10.1001/jamanetworkopen.2023.15885.
Please send us corrections, updates, or comments.
c19early involves the extraction of 100,000+ datapoints from
thousands of papers. Community updates
help ensure high accuracy.
Treatments and other interventions are complementary.
All practical, effective, and safe
means should be used based on risk/benefit analysis.
No treatment or intervention is 100% available and effective for all current
and future variants.
We do not provide medical advice. Before taking any medication,
consult a qualified physician who can provide personalized advice and details
of risks and benefits based on your medical history and situation. FLCCC and WCH
provide treatment protocols.