


Diet for COVID-19: real-time meta analysis of 28 studies
Abstract
Statistically significant lower risk is seen for ICU admission, hospitalization, progression, recovery, cases, and viral clearance. 24 studies from 23 independent teams in 10 countries show statistically significant
improvements.
Meta analysis using the most serious outcome reported shows
50% [41‑58%] lower risk. Results are similar for higher quality studies.
Results are robust — in exclusion sensitivity analysis 26 of 28
studies must be excluded to avoid finding statistically significant efficacy
in pooled analysis.
Studies analyze diet quality before infection, and use different definitions of diet quality.
No treatment or intervention
is 100% effective. All practical, effective, and safe means should be used
based on risk/benefit analysis.
{kind=link}
Highlights
A healthier diet reduces
risk for COVID-19 with very high confidence for hospitalization, cases, and in pooled analysis, low confidence for ICU admission, progression, recovery, and viral clearance, and very low confidence for mortality.
21st treatment shown effective with ≥3 clinical studies in
June 2021, now with p < 0.00000000001 from 28 studies.
Real-time updates and corrections,
transparent analysis with all results in the same format, consistent protocol
for 69
treatments, outcome specific analyses and combined evidence from all studies.
{kind=link}
{kind=link}
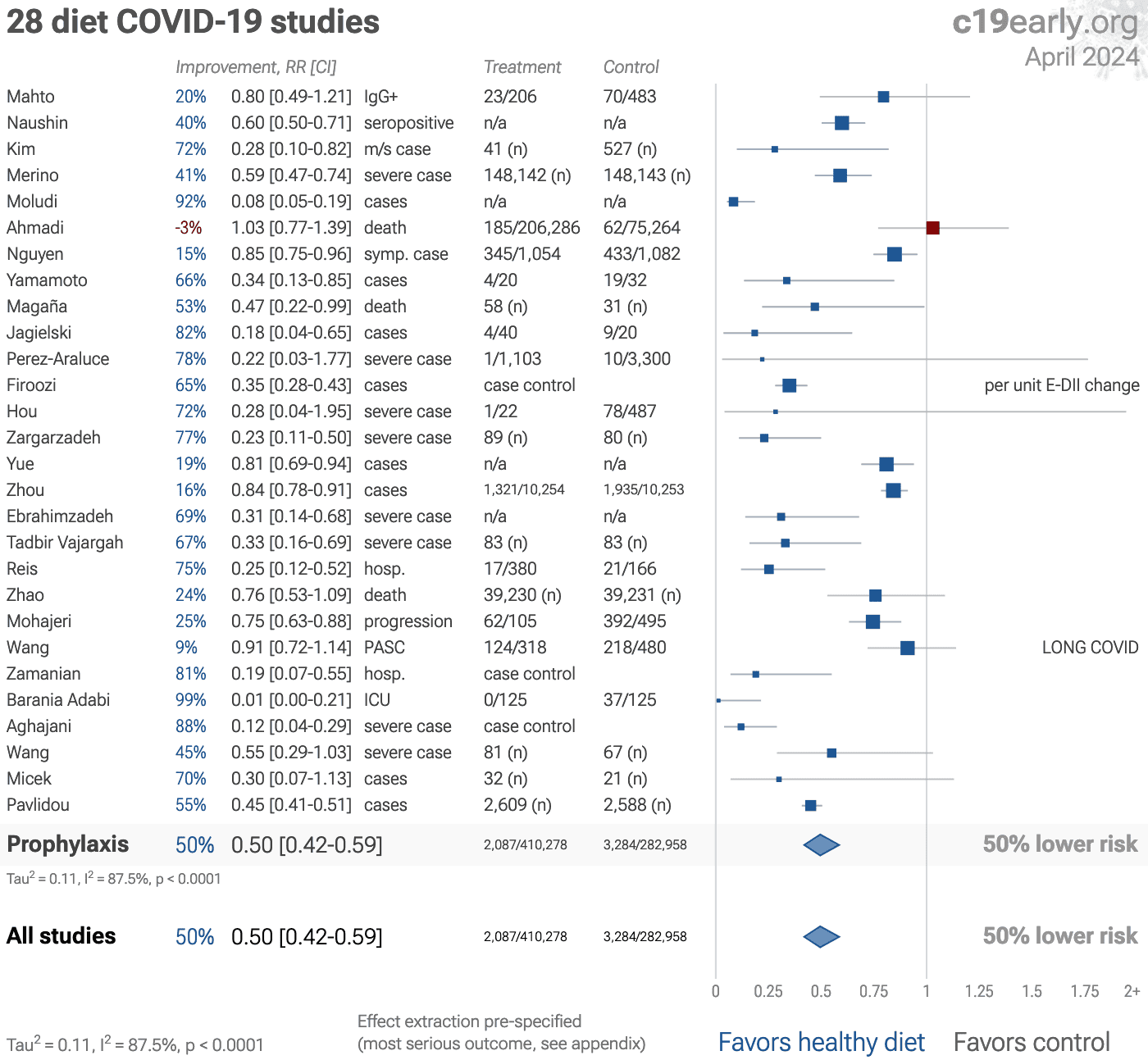
Figure 1.
A. Random effects
meta-analysis. This plot shows pooled effects,
see the specific outcome analyses for individual outcomes.
Analysis validating pooled outcomes for
COVID-19 can be found below.
Effect extraction is pre-specified, using the most serious outcome reported.
For details see the appendix.
B. Timeline of results in diet studies. The marked dates indicate the time when efficacy was known with a statistically significant improvement of ≥10% from ≥3 studies for pooled outcomes and one or more specific outcome. Efficacy based on specific outcomes was delayed by 3.4 months, compared to using pooled outcomes.
Improved diets contains many nutrients shown to be beneficial, enhance immune function, support a healthy gut microbiome, help regulate energy levels and metabolism, and reduce the risk of chronic diseases.
We analyze all significant
studies reporting COVID-19 outcomes as a function of diet quality and providing adjusted results.
Search methods, inclusion criteria, effect extraction criteria (more serious
outcomes have priority), all individual study data, PRISMA answers, and
statistical methods are detailed in Appendix 1. We present random
effects meta-analysis results for all studies, individual outcomes, and higher quality studies.
Table 1 summarizes the results for all studies, after exclusions, and for specific outcomes.
Figure 2, 3, 4, 5, 6, 7, 8, and 9
show forest plots for random effects meta-analysis of
all studies with pooled effects, mortality results, ICU admission, hospitalization, progression, recovery, cases, and viral clearance.
| Improvement | Studies | Patients | Authors | |
|---|---|---|---|---|
| All studies | 50% [41‑58%] **** | 28 | 693,236 | 358 |
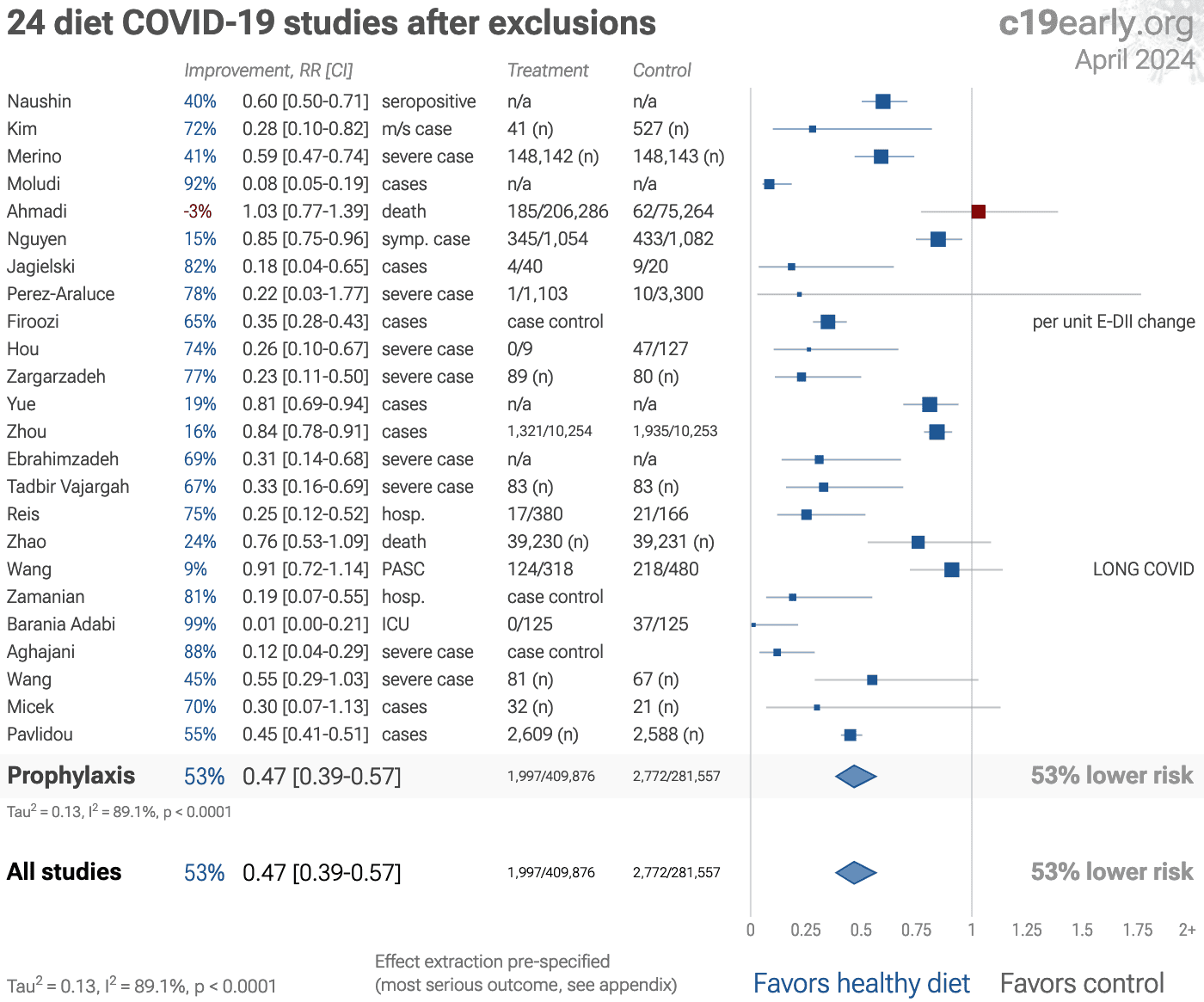
| After exclusions | 53% [43‑61%] **** | 24 | 691,433 | 340 |
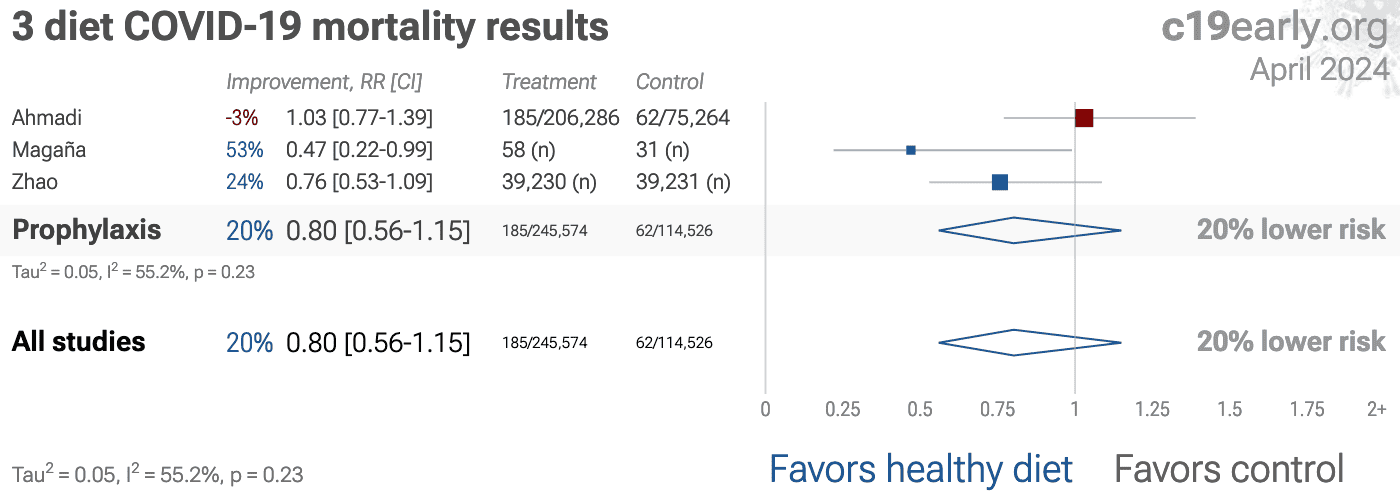
| Mortality | 20% [-15‑44%] | 3 | 360,100 | 20 |
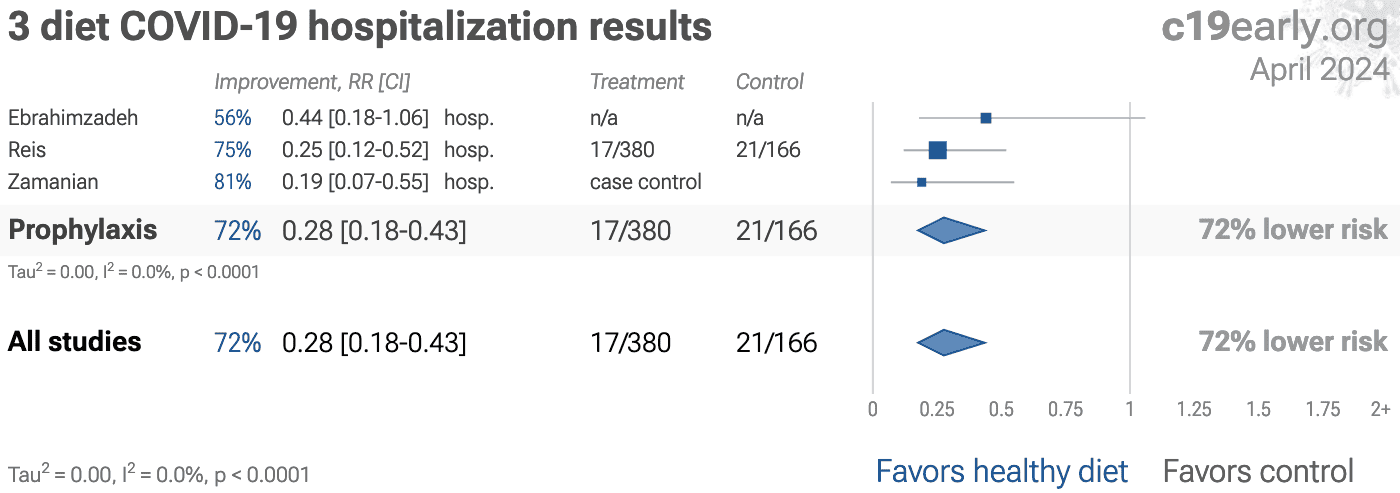
| HospitalizationHosp. | 72% [57‑82%] **** | 3 | 546 | 19 |
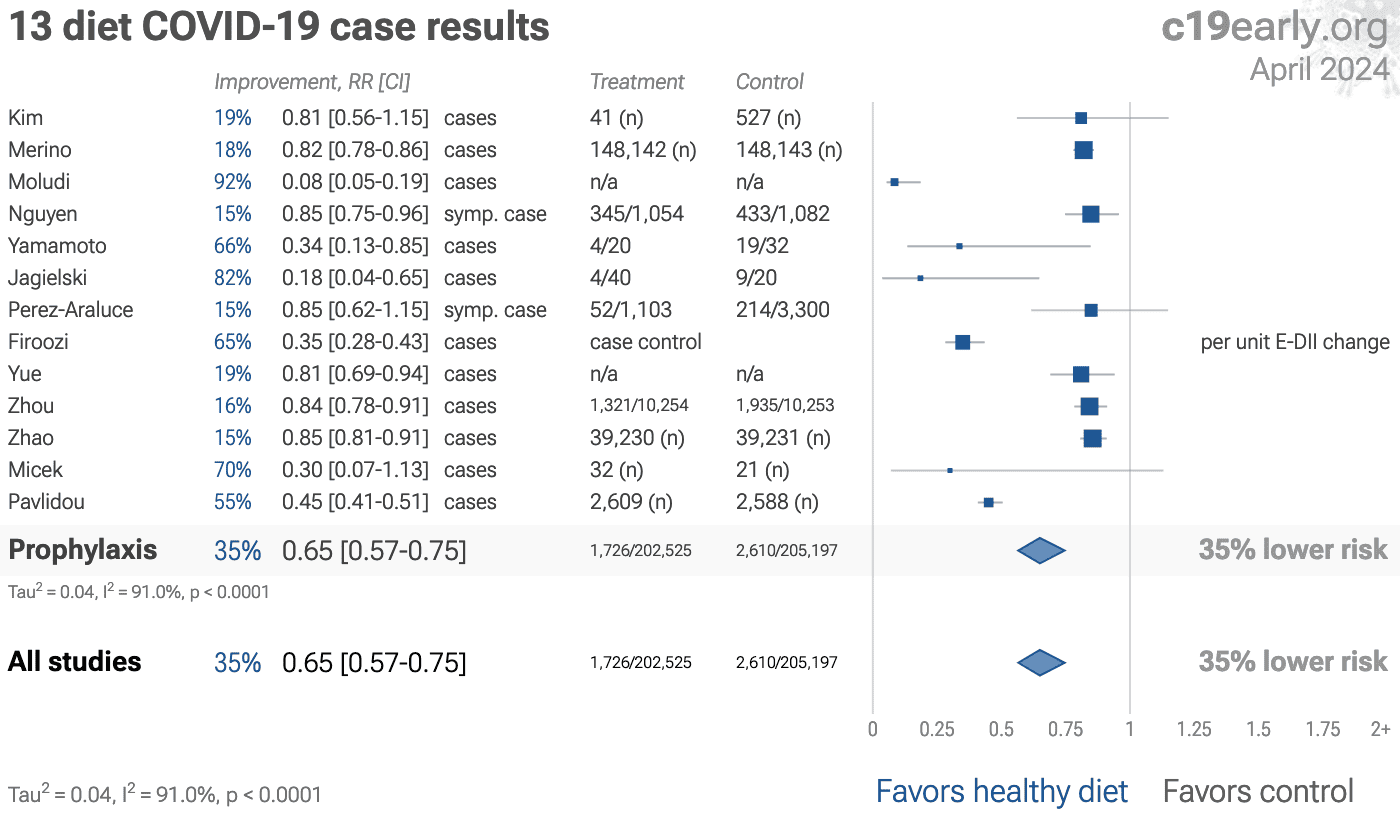
| Cases | 35% [25‑43%] **** | 13 | 407,722 | 132 |
Loading..
Loading..
Figure 2. Random effects meta-analysis for all studies.
This plot shows pooled effects,
see the specific outcome analyses for individual outcomes.
Analysis validating pooled outcomes for
COVID-19 can be found below.
Effect extraction is pre-specified, using the most serious outcome reported.
For details see the appendix.
{kind=link}
Loading..
Loading..
Figure 3. Random effects meta-analysis for mortality results.
{kind=link}
Loading..
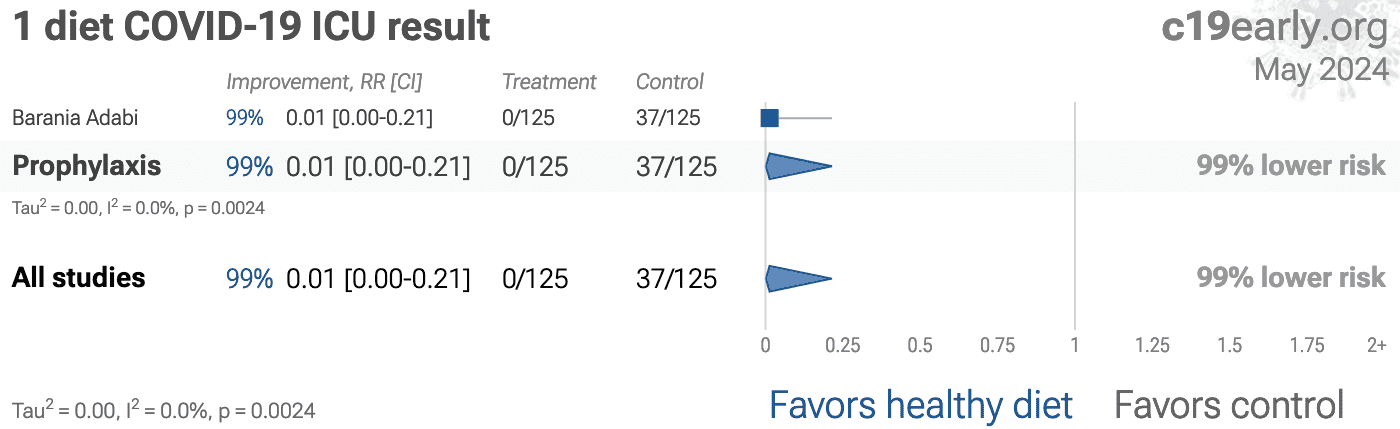
Figure 4. Random effects meta-analysis for ICU admission.
{kind=link}
Loading..
Figure 5. Random effects meta-analysis for hospitalization.
{kind=link}
Loading..
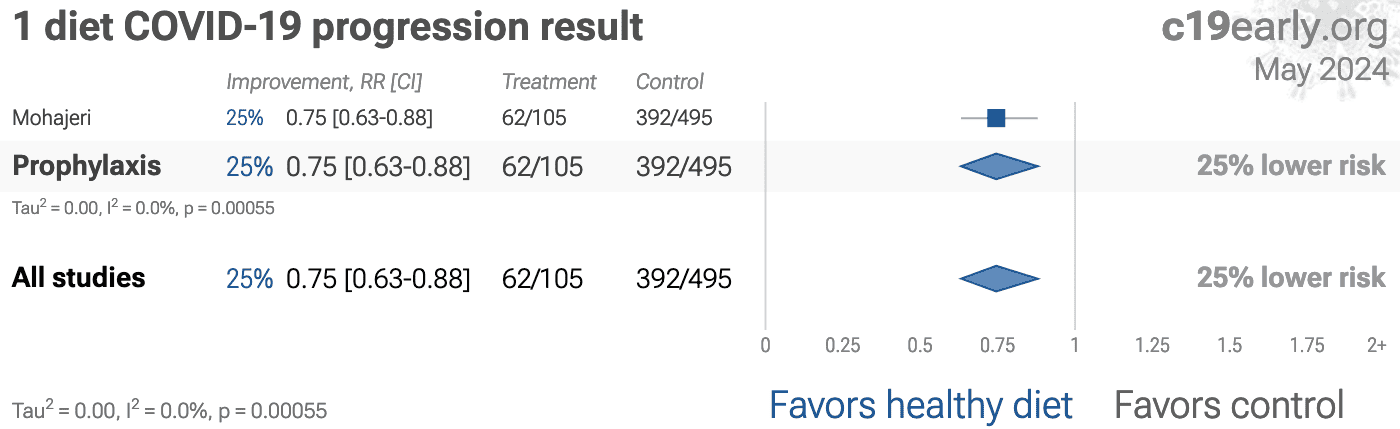
Figure 6. Random effects meta-analysis for progression.
{kind=link}
Loading..
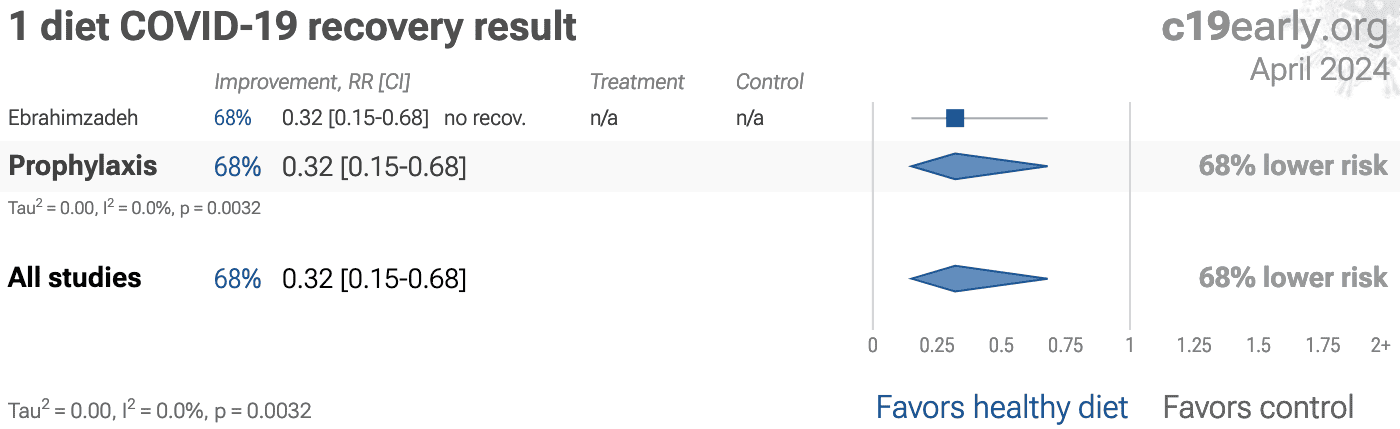
Figure 7. Random effects meta-analysis for recovery.
{kind=link}
Loading..
Figure 8. Random effects meta-analysis for cases.
{kind=link}
Loading..
Figure 9. Random effects meta-analysis for viral clearance.
To avoid bias in the selection of studies, we analyze all
non-retracted studies. Here we show the results after excluding
studies with major issues likely to alter results, non-standard studies, and
studies where very minimal detail is currently available. Our bias evaluation
is based on analysis of each study and identifying when there is a significant
chance that limitations will substantially change the outcome of the study. We
believe this can be more valuable than checklist-based approaches such as
Cochrane GRADE, which can be easily influenced by potential bias, may ignore
or underemphasize serious issues not captured in the checklists, and may
overemphasize issues unlikely to alter outcomes in specific cases (for example
certain specifics of randomization with a very large effect size and
well-matched baseline characteristics).
The studies excluded are as below.
Figure 10 shows a forest plot for random
effects meta-analysis of all studies after exclusions.
Hou, unadjusted results with no group details. Excluded results: severe case, moderate/severe case.
Magaña, unadjusted results with no group details.
Mahto, unadjusted results with no group details.
Mohajeri, unadjusted results with no group details.
Yamamoto, unadjusted results with no group details.
{kind=link}
Loading..
Figure 10. Random effects meta-analysis for all studies after exclusions.
This plot shows pooled effects,
see the specific outcome analyses for individual outcomes.
Analysis validating pooled outcomes for
COVID-19 can be found below.
Effect extraction is pre-specified, using the most serious outcome reported.
For details see the appendix.
For COVID-19, delay in clinical results translates into
additional death and morbidity, as well as additional economic and societal
damage. Combining the results of studies reporting different outcomes is
required.
There may be no mortality in a trial with low-risk patients,
however a reduction in severity or improved viral clearance may translate
into lower mortality in a high-risk population.
Different studies may report lower severity, improved recovery, and lower mortality,
and the significance may be very high when combining the results.
"The studies reported different outcomes"
is not a good reason for disregarding results.
We present both specific outcome and pooled analyses.
In order to combine the results of studies reporting different outcomes we use
the most serious outcome reported in each study, based on the thesis that
improvement in the most serious outcome provides comparable measures of
efficacy for a treatment. A critical advantage of this approach is
simplicity and transparency.
There are many other ways to combine evidence for different outcomes, along
with additional evidence such as dose-response relationships, however these
increase complexity.
Another way to view pooled analysis is that we are using more of
the available information. Logically we should, and do, use additional
information. For example dose-response and
treatment delay-response relationships provide significant additional evidence
of efficacy that is considered when reviewing the evidence for a
treatment.
Trials with high-risk patients may be restricted due to ethics for treatments
that are known or expected to be effective, and they increase difficulty for
recruiting. Using less severe outcomes as a proxy for more serious outcomes
allows faster collection of evidence.
For many COVID-19 treatments, a reduction in mortality logically
follows from a reduction in hospitalization, which follows from a reduction in
symptomatic cases, which follows from a reduction in PCR positivity. We can
directly test this for COVID-19.
Analysis of the the association between different outcomes across studies from
all 69
treatments we cover confirms the validity of pooled outcome analysis for COVID-19.
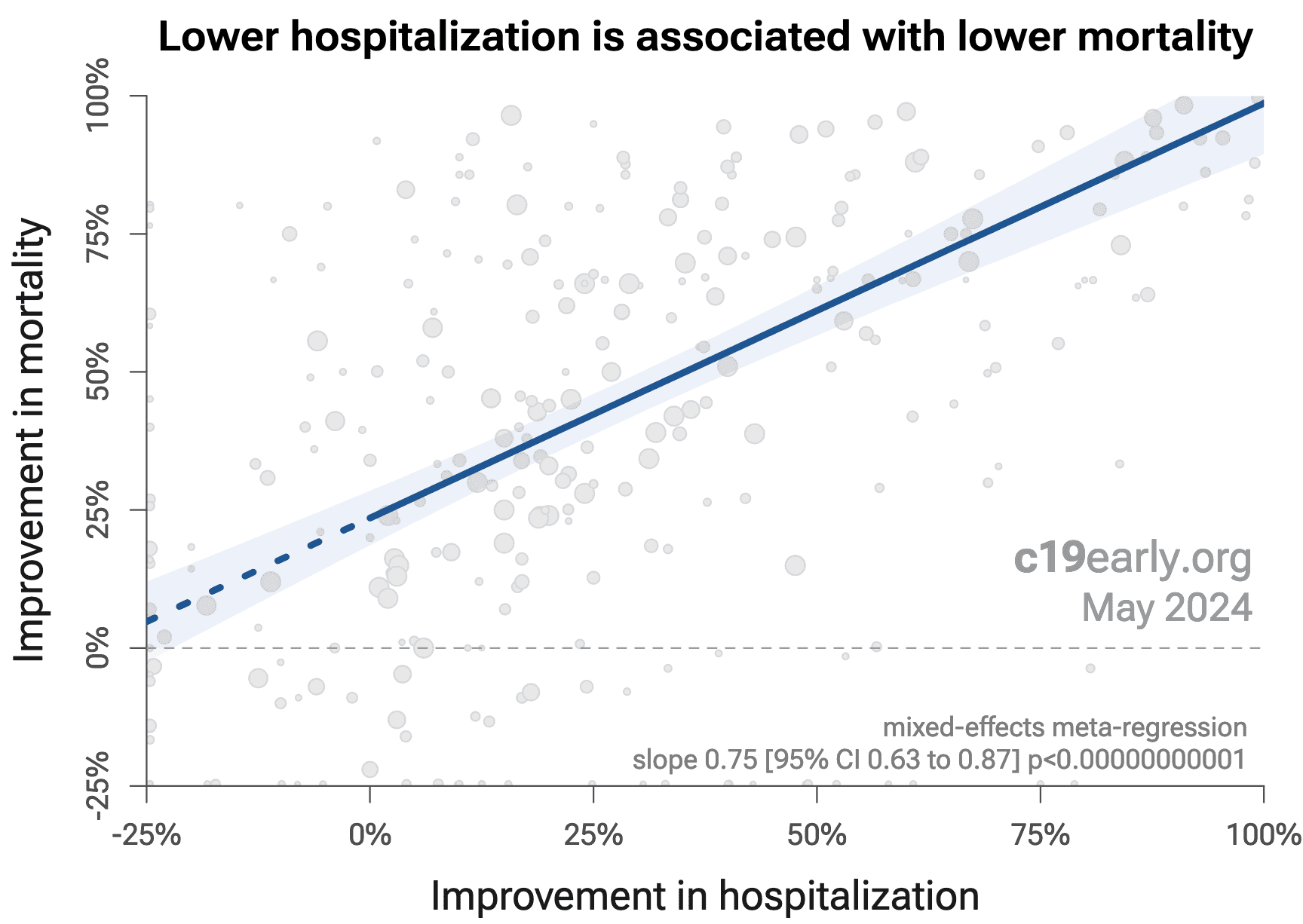
Figure 11 shows that lower hospitalization is very strongly associated
with lower mortality (p < 0.000000000001).
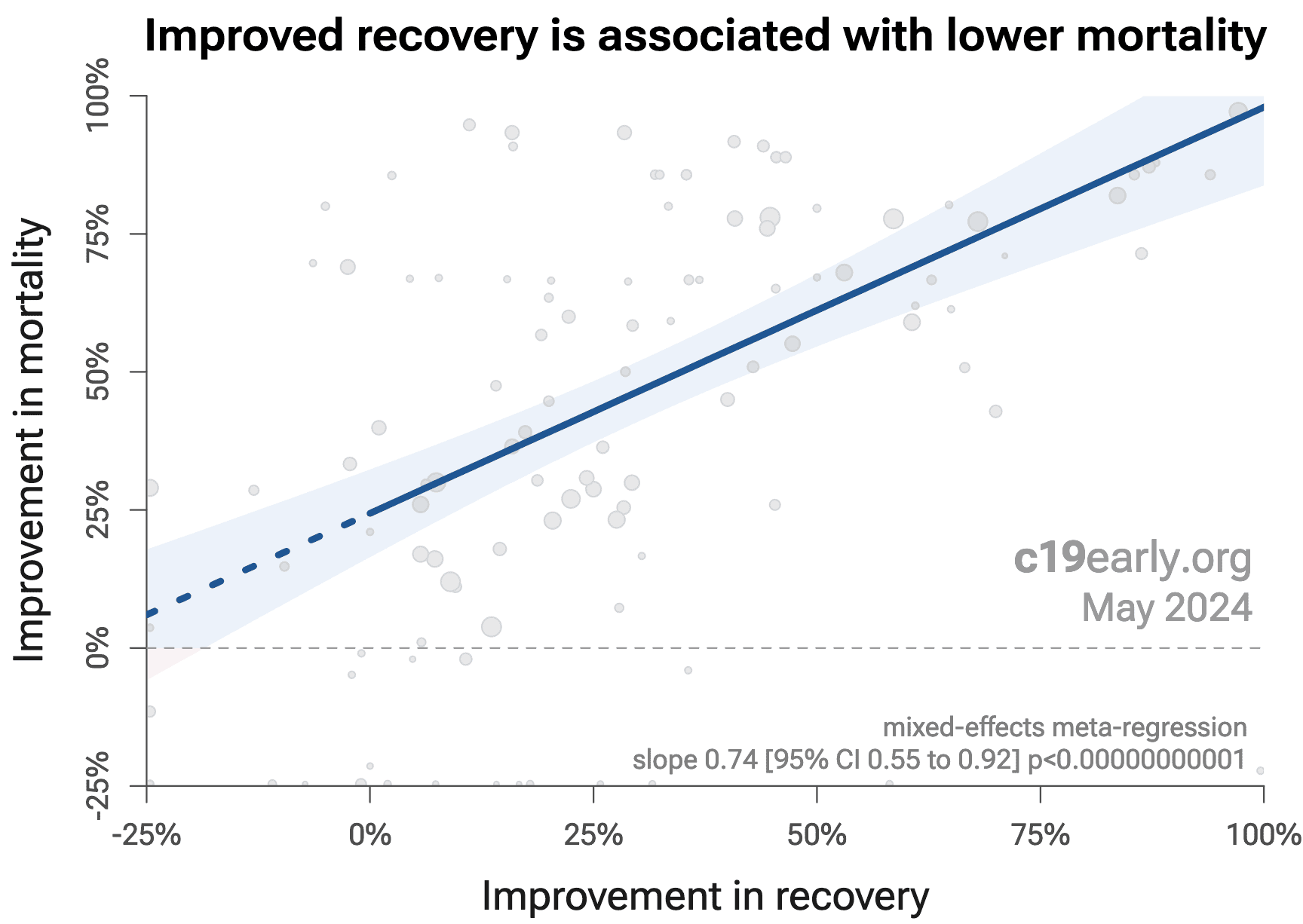
Similarly, Figure 12 shows that improved recovery is very strongly associated
with lower mortality (p < 0.000000000001).
Considering the extremes, Singh et al. show an association between viral clearance and
hospitalization or death, with p = 0.003 after excluding one large
outlier from a mutagenic treatment, and based on 44 RCTs including 52,384
patients.
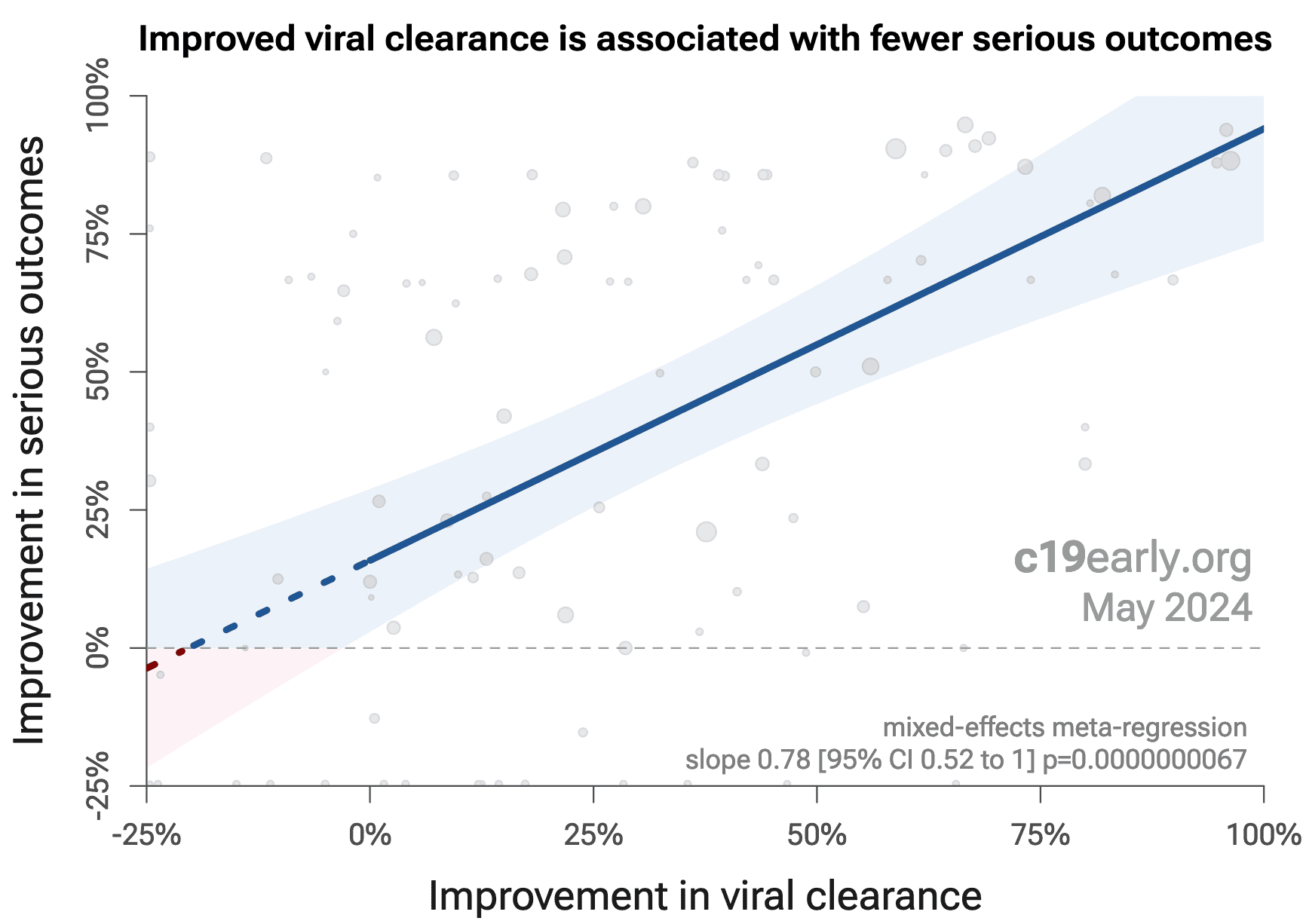
Figure 13 shows that improved viral clearance is strongly associated
with fewer serious outcomes. The association is very similar to
Singh et al., with higher confidence due to the larger number of
studies. As with Singh et al., the confidence increases
when excluding the outlier treatment, from p = 0.0000031 to p = 0.0000000067.
{kind=link}
Loading..
Figure 11. Lower hospitalization is associated with lower mortality, supporting pooled outcome analysis.
{kind=link}
Loading..
Figure 12. Improved recovery is associated with lower mortality, supporting pooled outcome analysis.
{kind=link}
Loading..
Figure 11. Improved viral clearance is associated with fewer serious outcomes, supporting pooled outcome analysis.
Currently, 44 of the treatments we analyze show statistically significant efficacy or harm, defined as ≥10% decreased risk or >0% increased risk from ≥3 studies. 88% of these have been confirmed with one or more specific outcomes, with a mean delay of 4.7 months. When restricting to RCTs only, 54% of treatments showing statistically significant efficacy/harm with pooled effects have been confirmed with one or more specific outcomes, with a mean delay of 5.5 months.
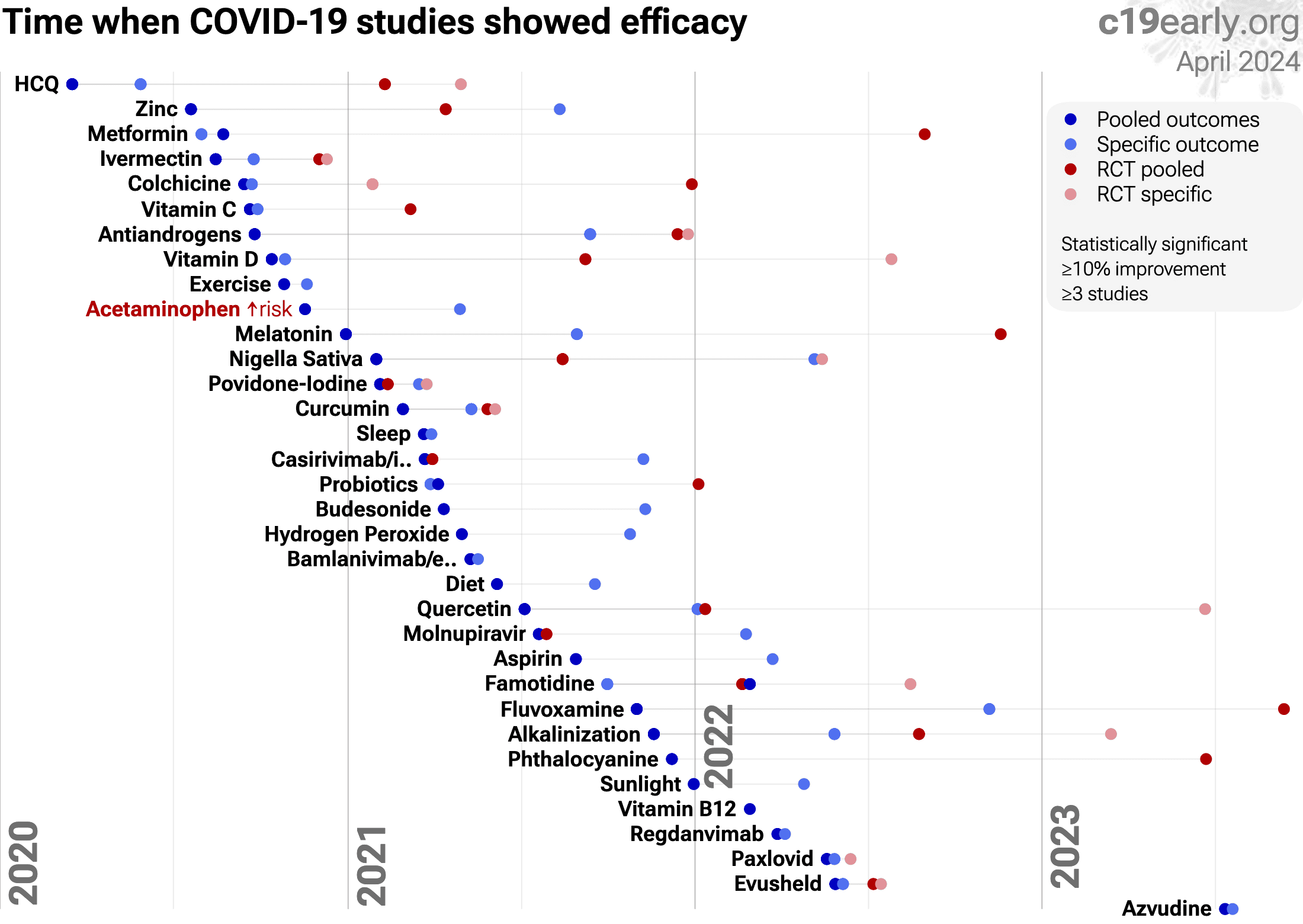
Figure 14 shows when treatments were found effective during the
pandemic. Pooled outcomes often resulted in earlier detection of efficacy.
{kind=link}
Loading..
Loading..
Figure 14. The time when studies showed that
treatments were effective, defined as statistically significant improvement of
≥10% from ≥3 studies.
Pooled results typically show efficacy earlier than specific
outcome results. Results from all studies often shows efficacy much earlier
than when restricting to RCTs.
Results reflect conditions as used in trials to date, these depend on the
population treated, treatment delay, and treatment regimen.
Pooled analysis could hide efficacy, for example a treatment that is
beneficial for late stage patients but has no effect on viral clearance may
show no efficacy if most studies only examine viral clearance. In practice, it
is rare for a non-antiviral treatment to report viral clearance and to not
report clinical outcomes; and in practice other sources of heterogeneity such
as difference in treatment delay is more likely to hide efficacy.
Analysis validates the use of pooled effects and shows significantly faster
detection of efficacy on average.
However, as with all meta analyses, it is important to review the different
studies included. We also present individual outcome analyses, which may be
more informative for specific use cases.
Currently all studies are peer-reviewed.
Other meta analyses show significant improvements with diet for hospitalization Rahmati, severity Hao, and cases Hao, Rahmati.
Kahleova et al. present a review covering diet for COVID-19.
SARS-CoV-2 infection and replication involves a complex interplay of 50+ host
and viral proteins and other factors Lui, Lv, Malone, Murigneux, Niarakis,
providing many therapeutic targets.
Over 7,000 compounds have been predicted to reduce COVID-19
risk c19early.org, either by directly
minimizing infection or replication, by supporting immune system function, or
by minimizing secondary complications.
Improved diets contains many nutrients shown to be beneficial, enhance immune function, support a healthy gut microbiome, help regulate energy levels and metabolism, and reduce the risk of chronic diseases.
Figure 15 shows an overview of the results for diet
in the context of multiple COVID-19 treatments, and Figure 16 shows a plot
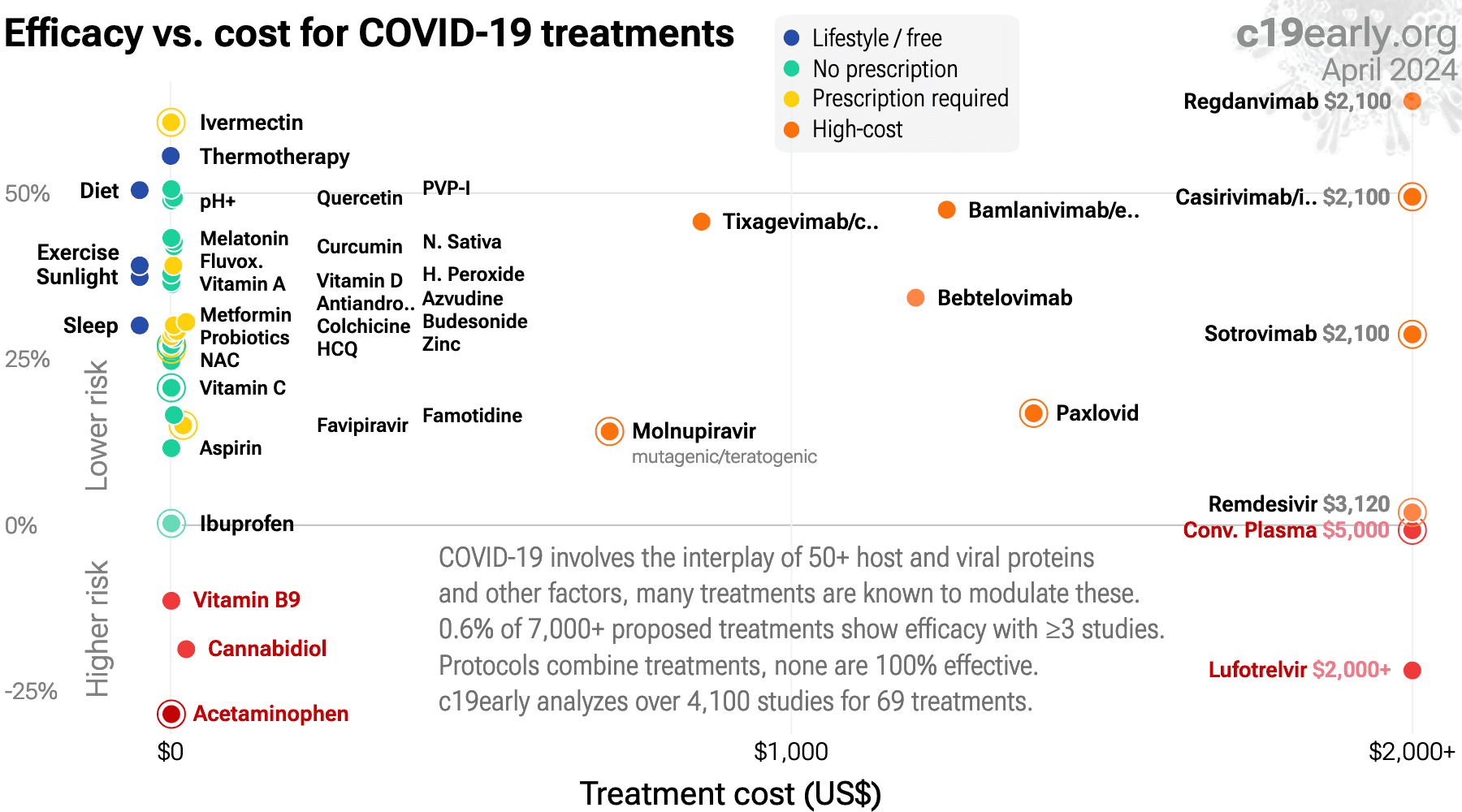
of efficacy vs. cost for COVID-19 treatments.
{kind=link}
Loading..
Figure 15.
Scatter plot showing results within the context of multiple COVID-19 treatments.
Diamonds shows the results of random effects meta-analysis.
0.6% of 7,000+ proposed treatments show efficacy
c19early.org (B).
{kind=link}
Loading..
Loading..
Figure 16. Efficacy vs. cost for COVID-19 treatments.
Improved diets contains many nutrients shown to be beneficial, enhance immune function, support a healthy gut microbiome, help regulate energy levels and metabolism, and reduce the risk of chronic diseases.
People with healthier diets have reduced risk for COVID-19.
Statistically significant lower risk is seen for ICU admission, hospitalization, progression, recovery, cases, and viral clearance. 24 studies from 23 independent teams in 10 countries show statistically significant
improvements.
Meta analysis using the most serious outcome reported shows
50% [41‑58%] lower risk. Results are similar for higher quality studies.
Results are robust — in exclusion sensitivity analysis 26 of 28
studies must be excluded to avoid finding statistically significant efficacy
in pooled analysis.
Studies analyze diet quality before infection, and use different definitions of diet quality.
{kind=link}
Aghajani:
Case control study of 295 COVID-19 patients in Iran, showing lower risk of severe cases with higher dietary antioxidant quality scores, and with higher intake of vitamin D.
{kind=link}
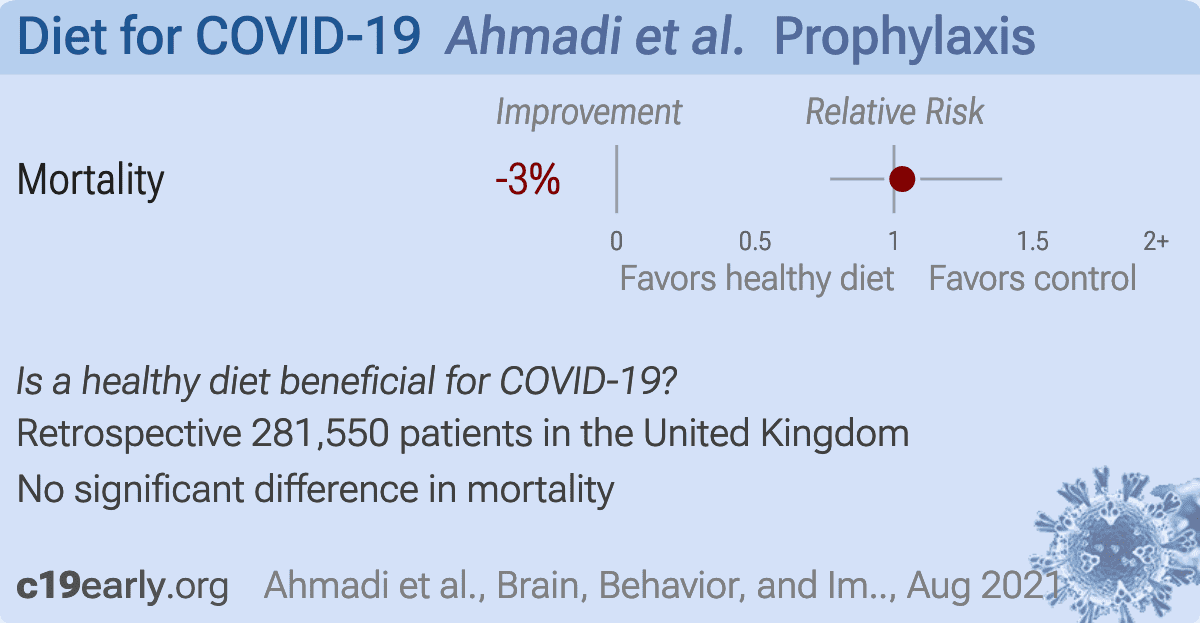
Ahmadi:
Retrospective 468,569 adults in the UK, showing significantly lower COVID-19 mortality with physical activity.
{kind=link}
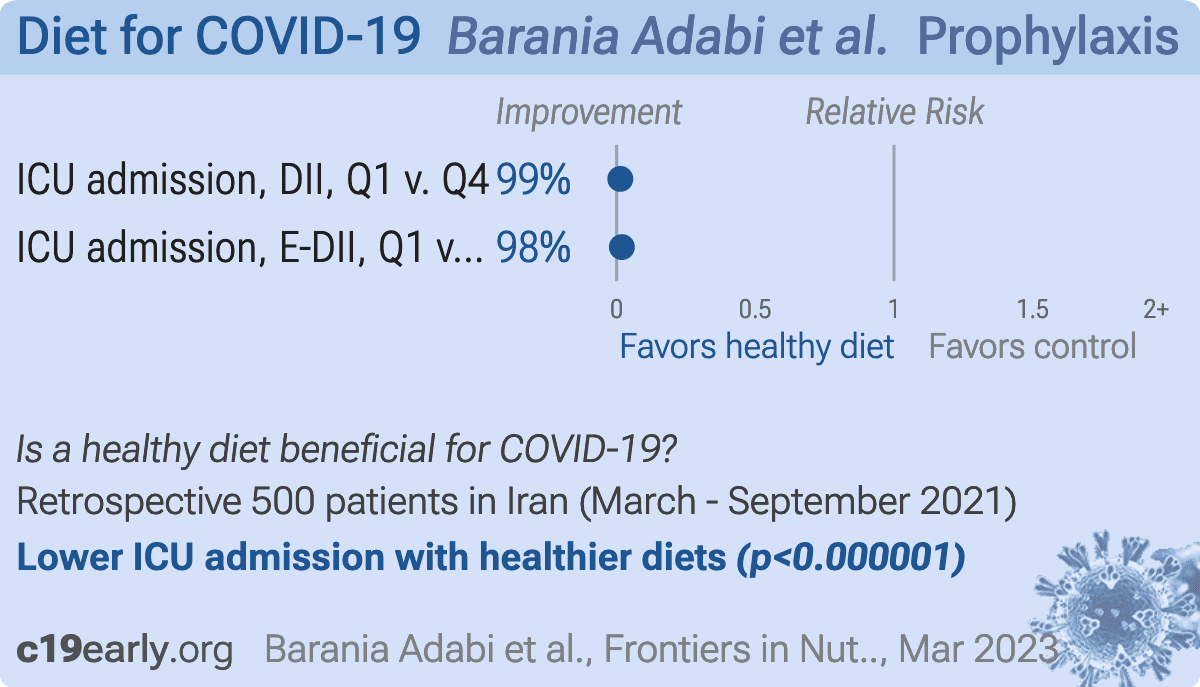
Barania Adabi:
Retrospective 500 COVID-19 patients, showing dietary inflammatory index (DII) and energy-adjusted dietary inflammatory index (E-DII) associated with COVID-19 severity.
{kind=link}
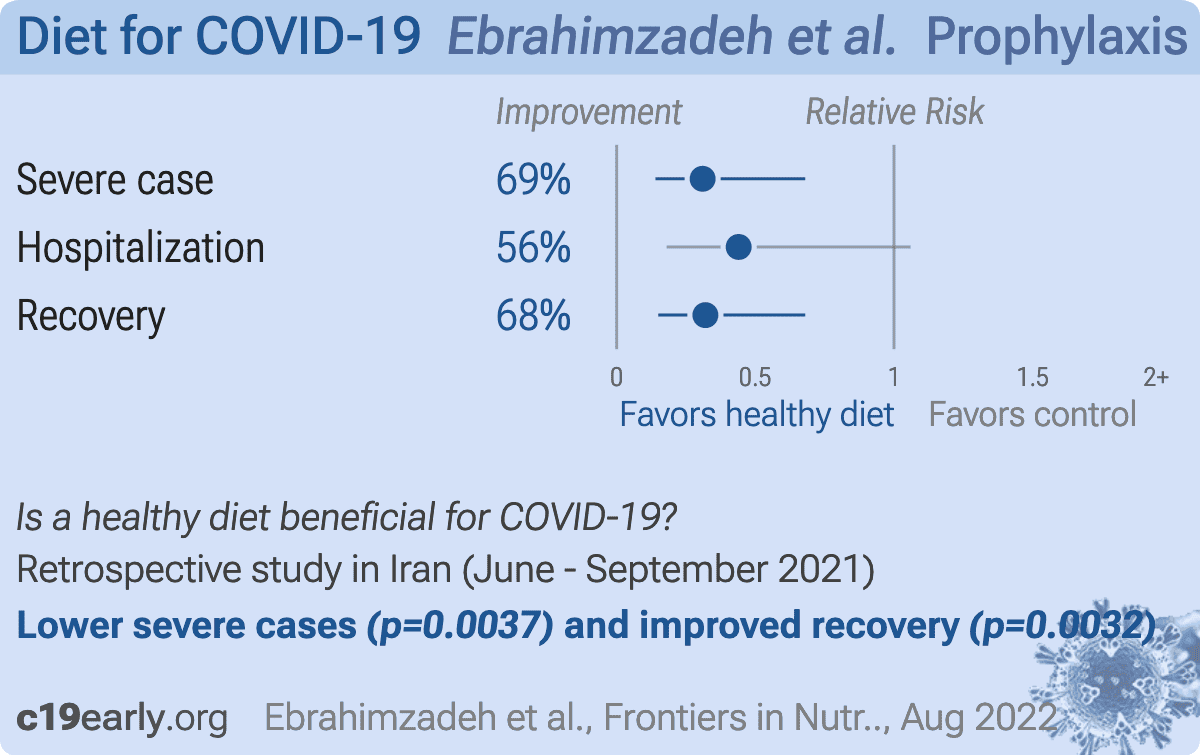
Ebrahimzadeh:
Retrospective 250 recovered COVID-19 patients, showing lower risk of severe cases and shorter recovery and hospitalization times with a healthy diet.
Notably, all individual symptoms show lower incidence with a healthy diet with the exception of fever and chills. Fever and chills help the immune system fight infections (shivering helps to raise the body temperature).
Notably, all individual symptoms show lower incidence with a healthy diet with the exception of fever and chills. Fever and chills help the immune system fight infections (shivering helps to raise the body temperature).
{kind=link}
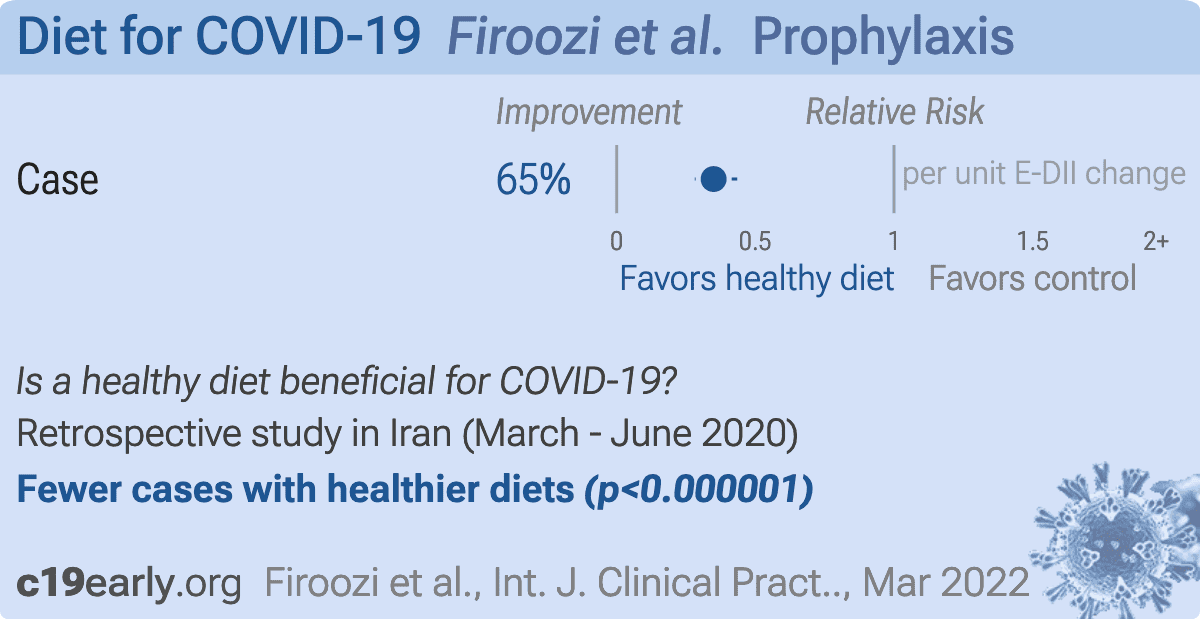
Firoozi:
Retrospective 133 COVID-19 patients and 322 controls, showing higher risk of COVID-19 for diets that have a higher inflammatory index (E-DII).
{kind=link}
Hou:
Retrospective 509 COVID-19 patients in Taiwan, showing higher risk of critical COVID-19 cases with non-vegetarian diets.
{kind=link}
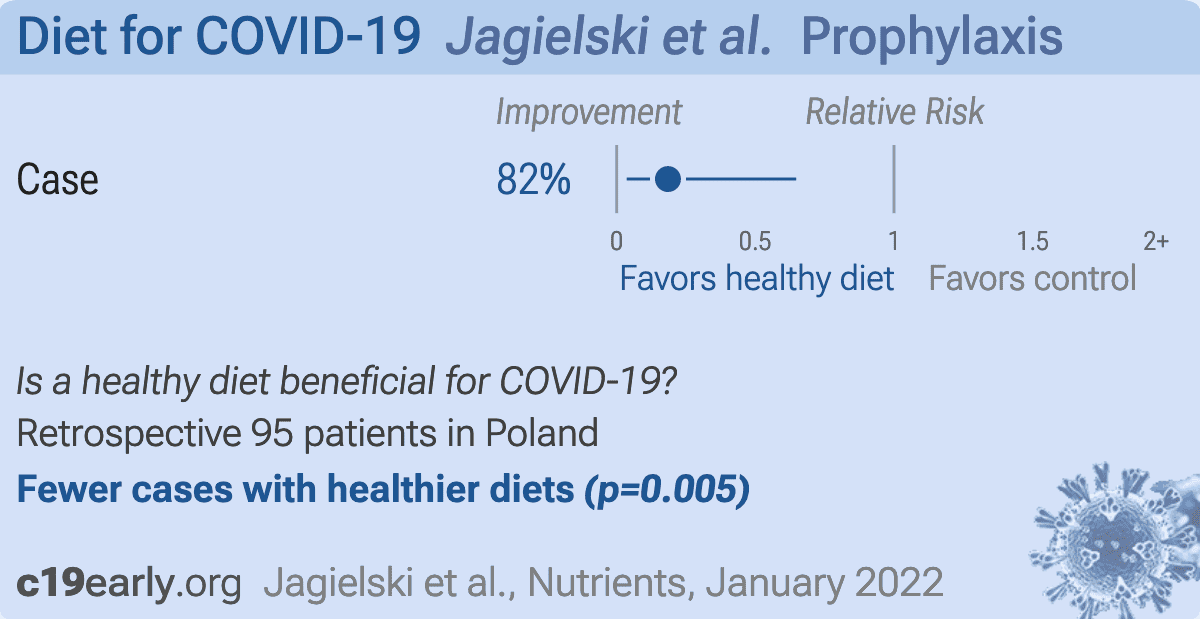
Jagielski:
Retrospective 95 people in Poland, showing significantly lower risk of COVID-19 with higher consumption of fruits, vegetables, and nuts. Diets with higher consumption of fruits, vegetables, and nuts had a significantly lower dietary inflammatory index.
{kind=link}
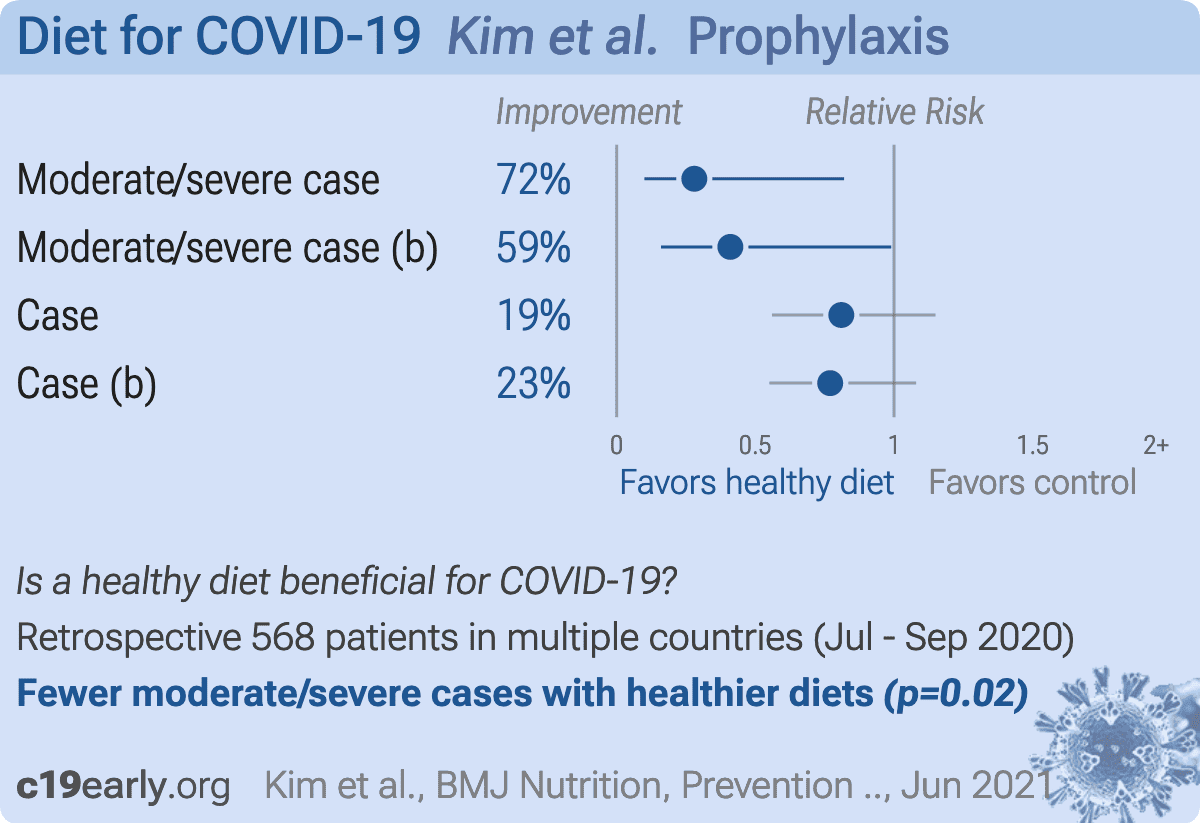
Kim:
Retrospective healthcare workers in six countries with exposure to COVID-19 patients, showing lower risk of moderate/severe COVID-19 with plant-based diets.
{kind=link}
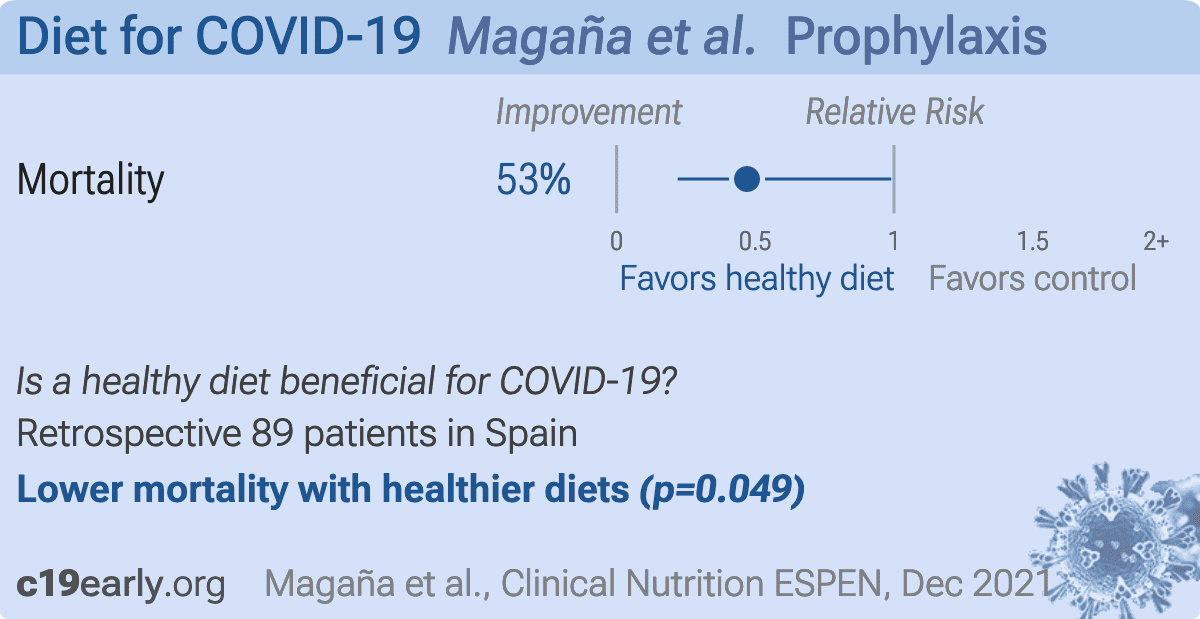
Magaña:
Retrospective 89 COVID-19 patients in Spain, showing lower mortality with adherence to the Mediterranean diet.
{kind=link}
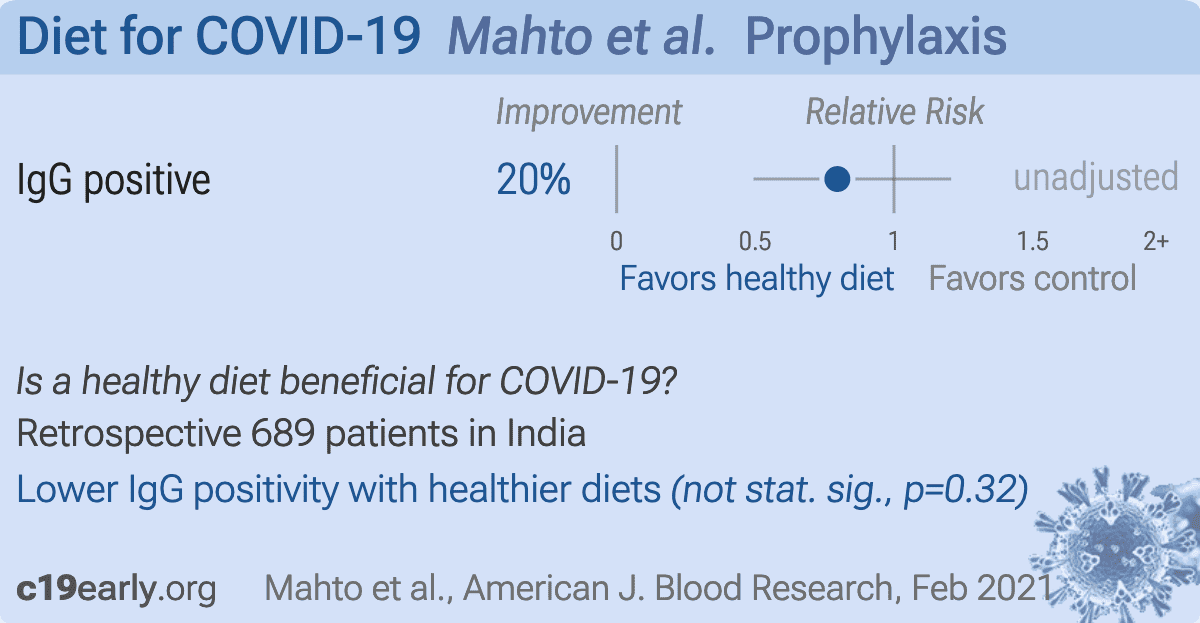
Mahto:
Retrospective 689 healthcare workers in India, showing non-statistically significant lower risk of IgG positivity with a vegetarian diet in unadjusted results.
{kind=link}
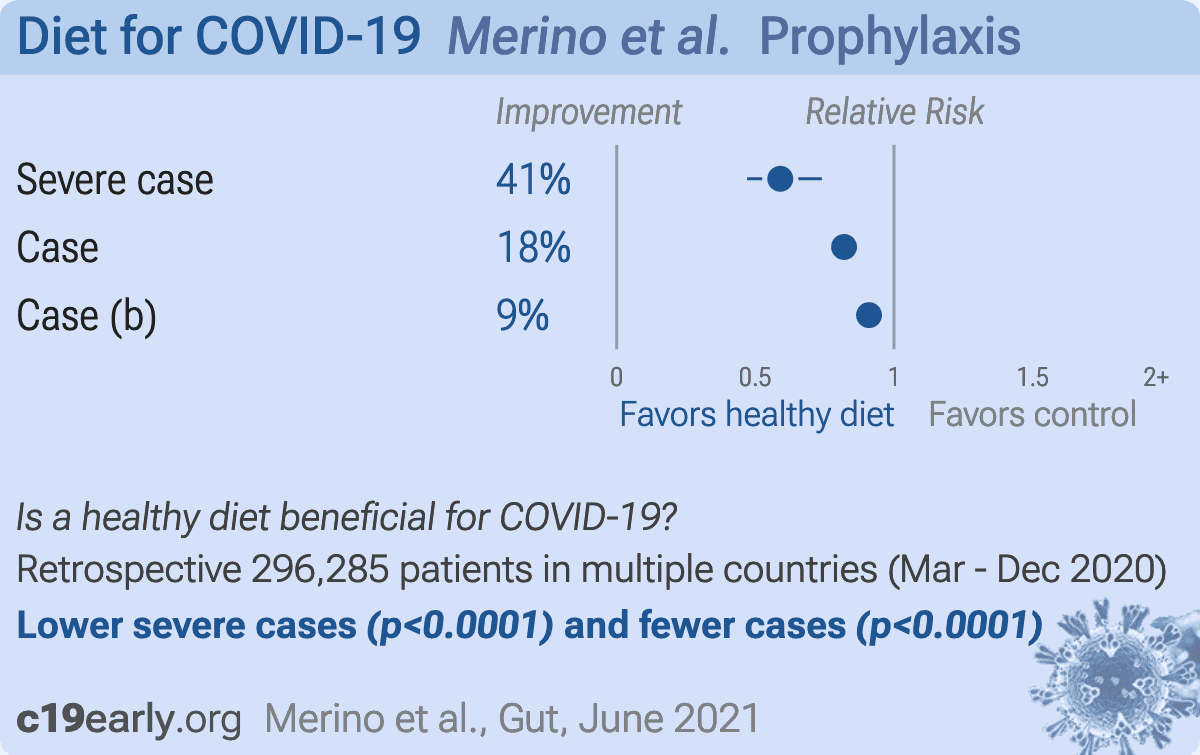
Merino:
Retrospective 592,571 participants in the UK and USA with 31,815 COVID-19 cases, showing lower risk or COVID-19 cases and severity for higher healthful plant-based diet scores. Notably, the assocation was less evident with higher levels of physical activity.
{kind=link}
Micek:
Dietary analysis of 95 adults in Poland, showing lower risk of COVID-19 with higher intake of polyphenols, lignans, and phytosterols. Results were statistically significant for total phytosterols, secoisolariciresinol, β-sitosterol, matairesinol, and stigmasterol. Authors suggest that beneficial effects on gut microbiota and immune function may contribute to the lower risk.
{kind=link}
Mohajeri:
Retrospective 600 COVID-19 patients in Iran with moderate/severe CT scans, showing lower prevalence of dyspnea, fever, taste/smell abnormalities, and cough with high adherence to the Mediterranean diet in unadjusted results.
{kind=link}
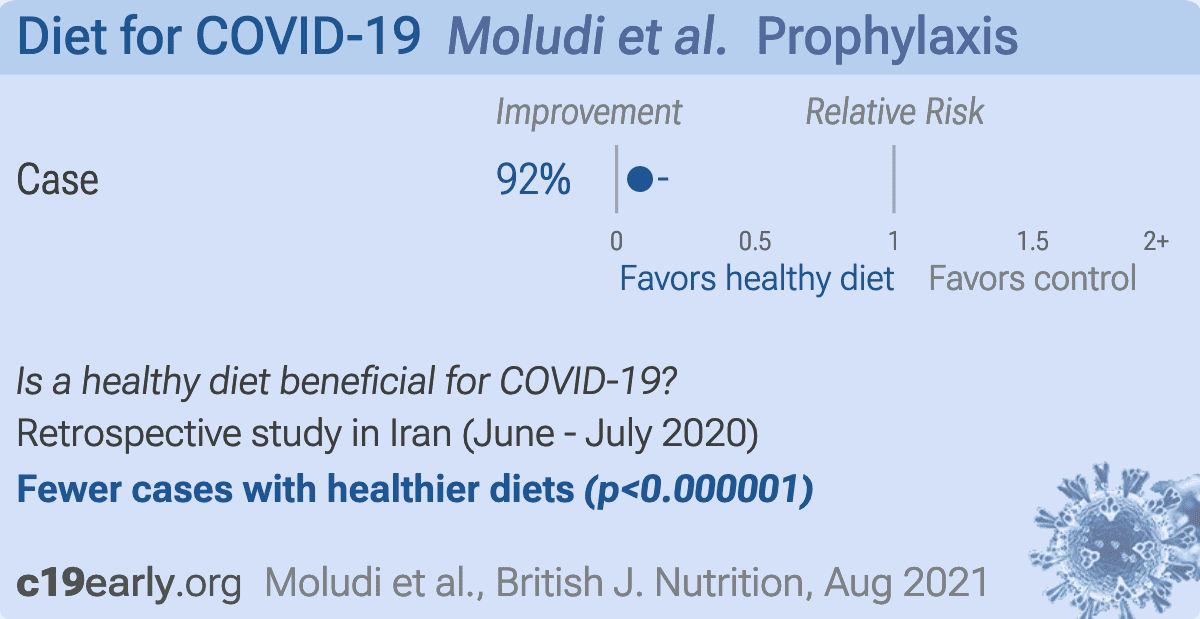
Moludi:
Retrospective 60 COVID-19 hospitalized patients and 60 controls in Iran, showing pro-inflammatory diets associated with COVID-19 cases and severity. IR.KUMS.REC.1399·444, IR.TBZMED.REC.1399·225.
{kind=link}
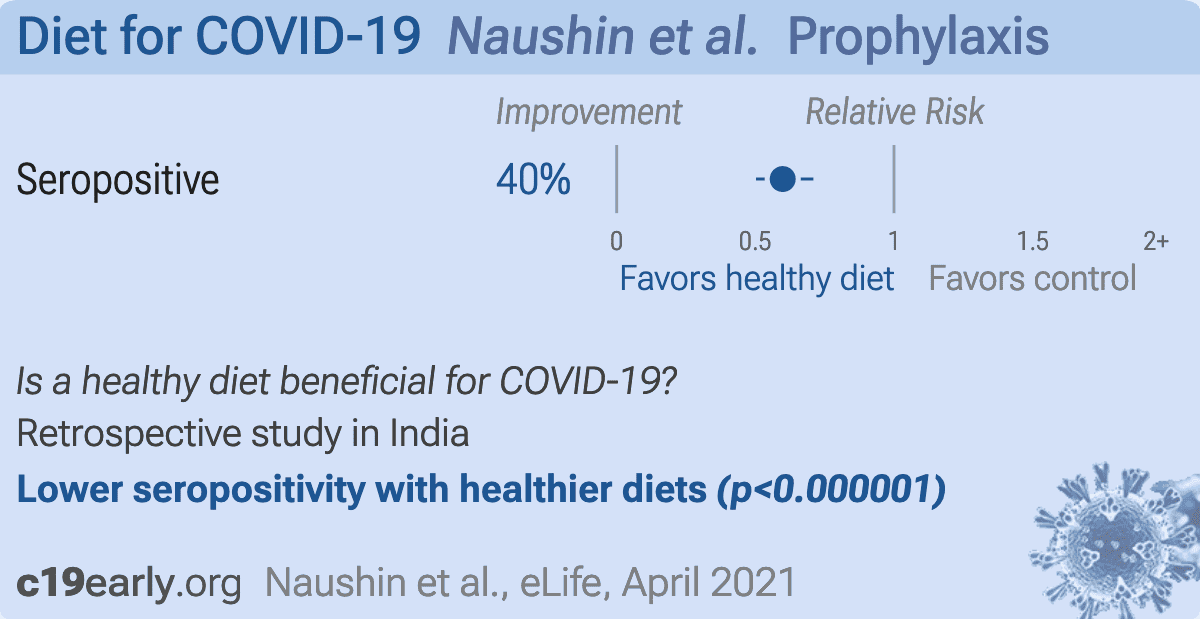
Naushin:
Retrospective 10,427 volunteers in India, 1,058 anti-nucleocapsid antibody positive, showing lower risk of seropositivity with a vegetarian diet.
{kind=link}
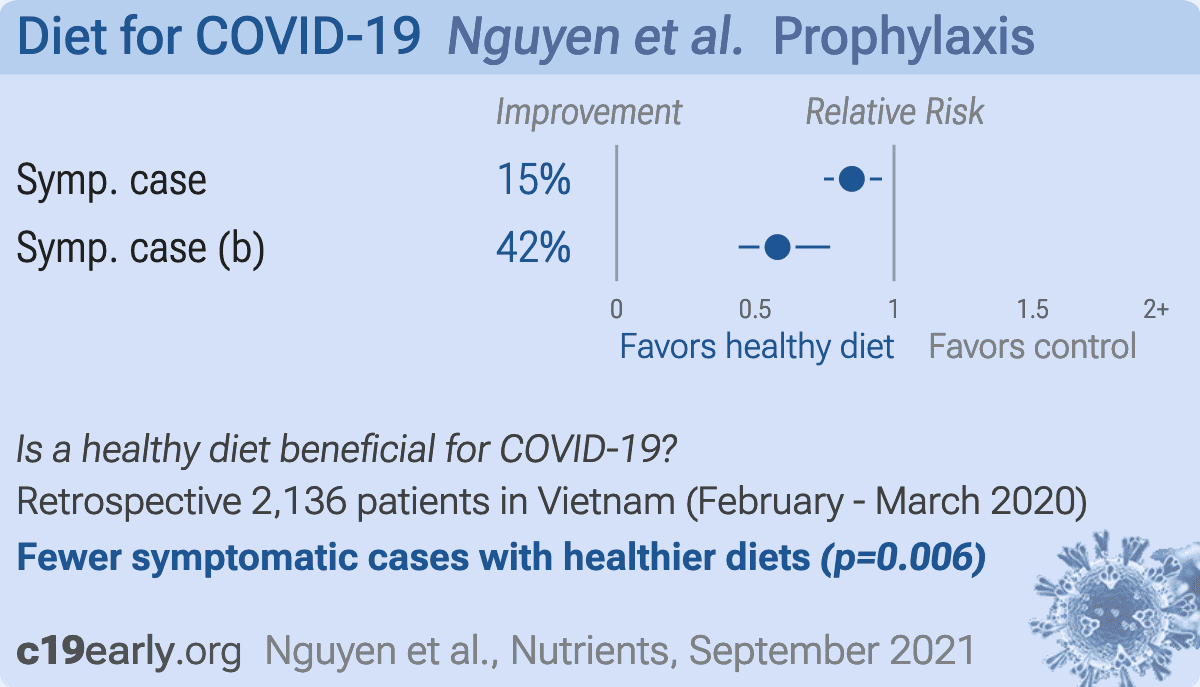
Nguyen:
Analysis of 3,947 participants in Vietnam, showing significantly lower risk of COVID-19-like symptoms with physical activity and with a healthy diet. The combination of being physically active and eating healthy reduced risk further compared to either alone. The analyzed period was Feb 14 to Mar 2, 2020, which may have been before testing was widely available.
{kind=link}
Pavlidou:
Retrospective 5,197 Greek adults over 65. After adjustment for confounders, COVID-19 infection was independently associated with poor sleep, low physical activity, low Mediterranean diet adherence, living in urban areas, smoking, obesity, depression, anxiety, stress, and poor health-related quality of life.
{kind=link}
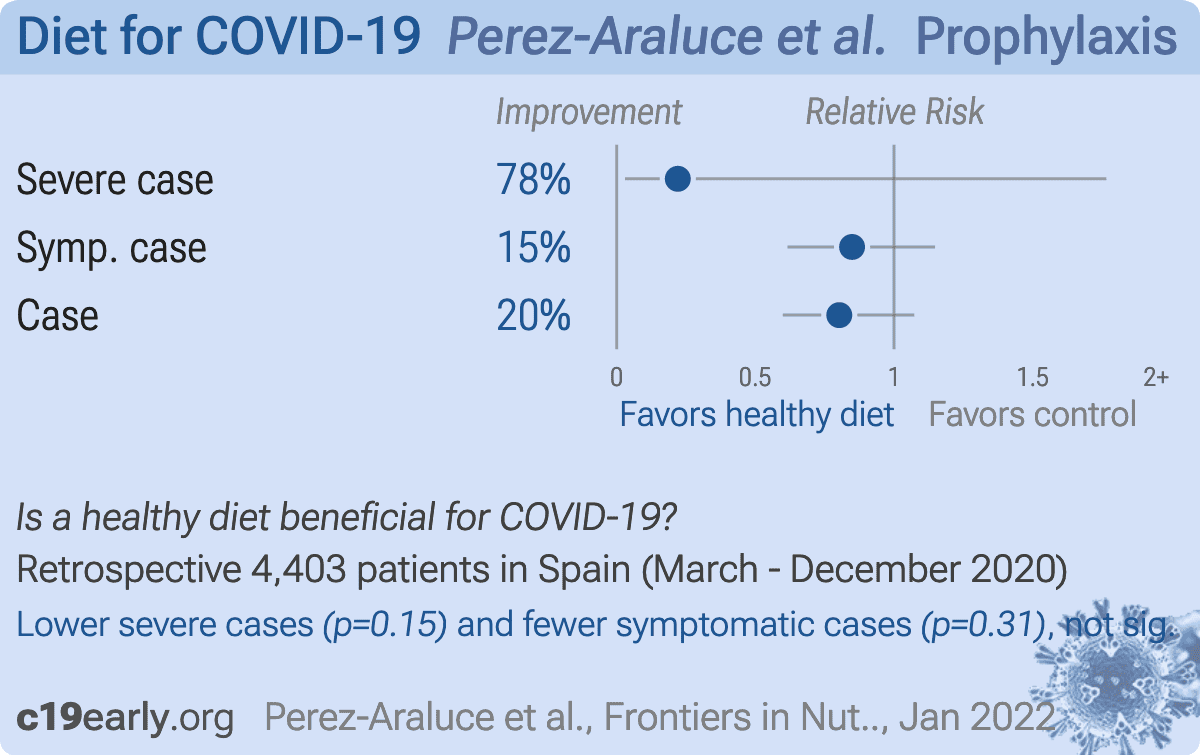
Perez-Araluce:
Retrospective 5,194 participants in Spain with 382 COVID-19 cases, showing lower risk of COVID-19 with high adherence to a Mediterranean diet, with statistical significance only when excluding healthcare professionals.
{kind=link}
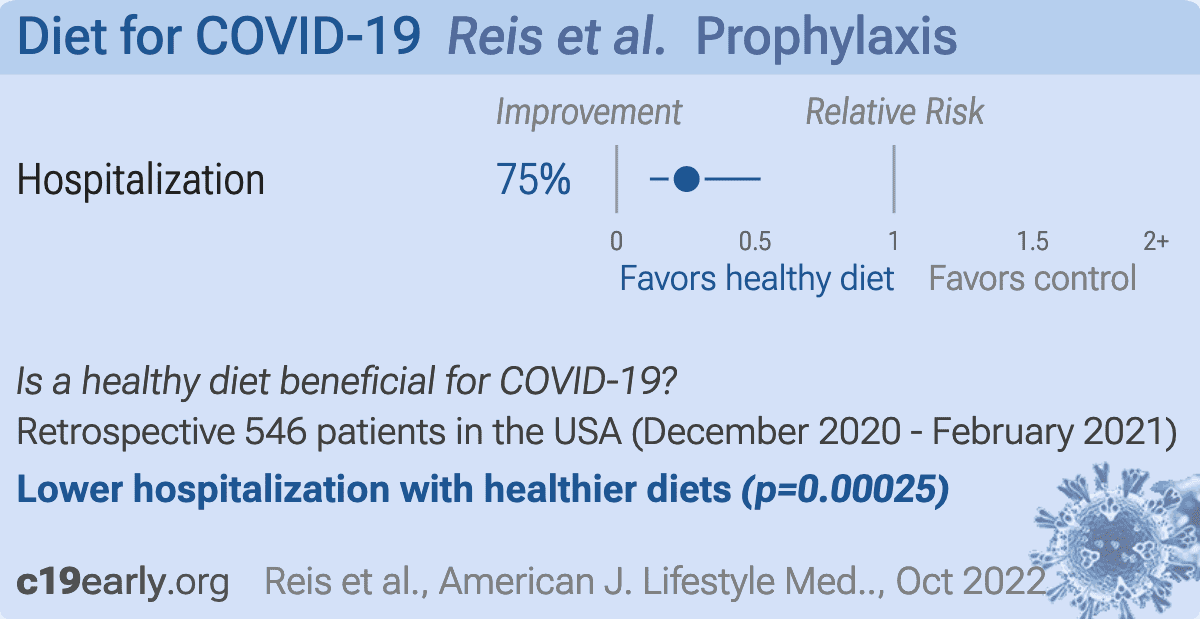
Reis:
Retrospective 546 COVID+ patients in the USA, showing lower risk of hospitalization with higher consumption of vegetables.
{kind=link}
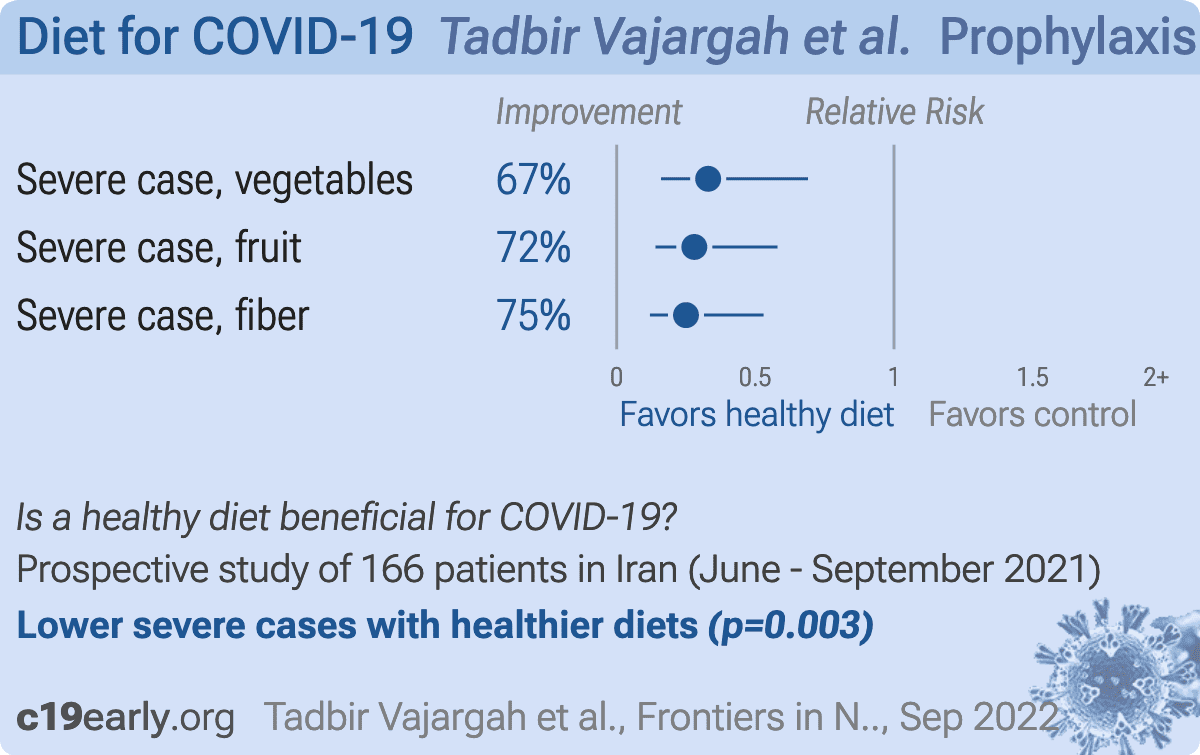
Tadbir Vajargah:
Retrospective 250 hospitalized patients in Iran, showing higher consumption of fruits, vegetables, and fiber associated with lower COVID-19 severity.
Tomasa-Irriguible:
Estimated 300 patient diet early treatment RCT with results expected soon (estimated completion over 4 months ago).
{kind=link}
Wang:
Retrospective 148 hospitalized COVID-19 patients in China, showing lower severity and faster viral clearance with improved nutrition.
{kind=link}
Wang (B):
Prospective analysis of 32,249 women from the Nurses’ Health Study II in the USA, showing lower risk of PASC with a healthy lifestyle, and in a dose-dependent manner. Participants with 5 or 6 healthy lifestyle factors had significantly lower COVID-19 hospitalization and PASC. BMI and sleep were independently associated with risk of PASC.
{kind=link}
Yamamoto:
Retrospective 84 flight attendants, 52 reporting COVID-19 status and diet quality, showing higher risk of COVID-19 with lower self-reported diet quality.
{kind=link}
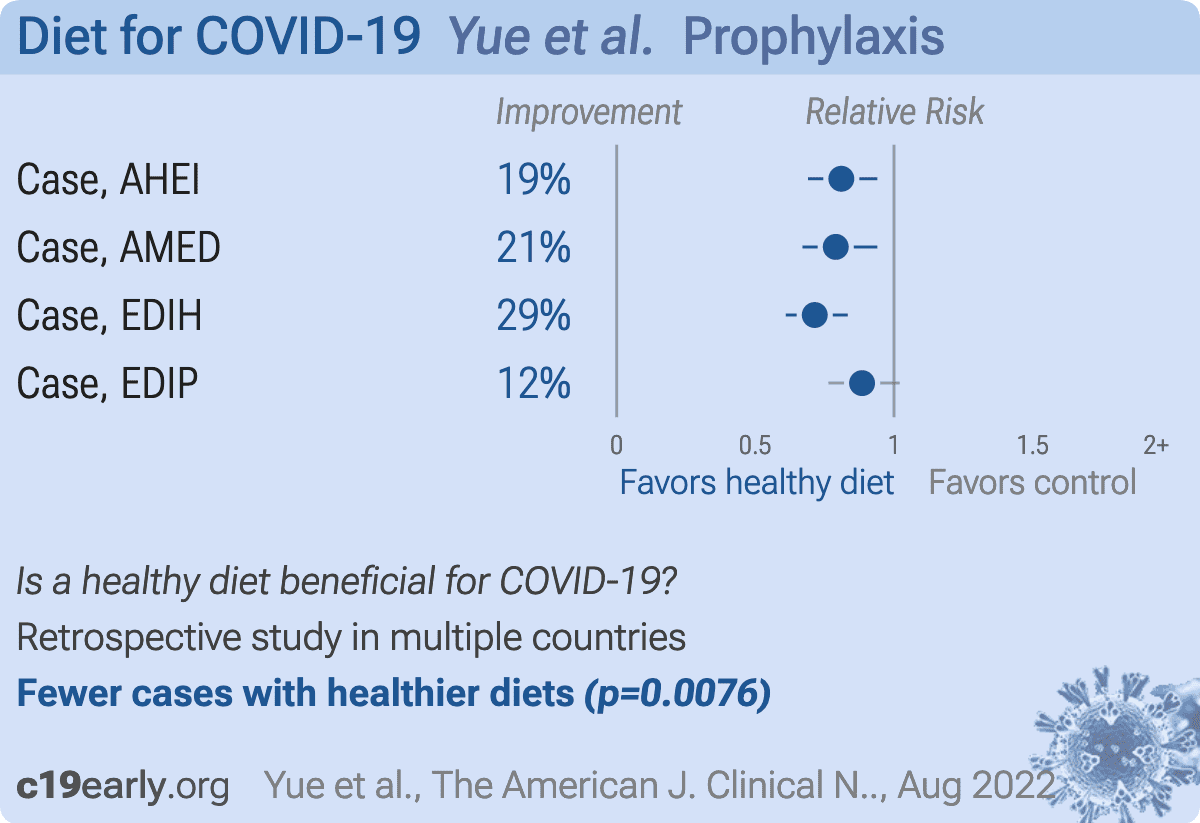
Yue:
Analysis of 42,935 participants showing lower risk of COVID-19 with healthier diets. Risk of severe cases was also lower with healthier diets, while not reaching statistical significance. Severity results are only provided with diet indices as a continuous variable.
{kind=link}
Zamanian:
Case control study with 53 inpatients and 88 outpatients in Iran, showing lower risk of hospitalization with increased adherence to the DASH (Dietary Approach to Stop Hypertension) diet. Increased intake of fruits, vegetables and low-fat dairy products, and lower intake of sodium and processed/red meat were significantly associated with reduced risk of hospitalization due to COVID-19.
{kind=link}
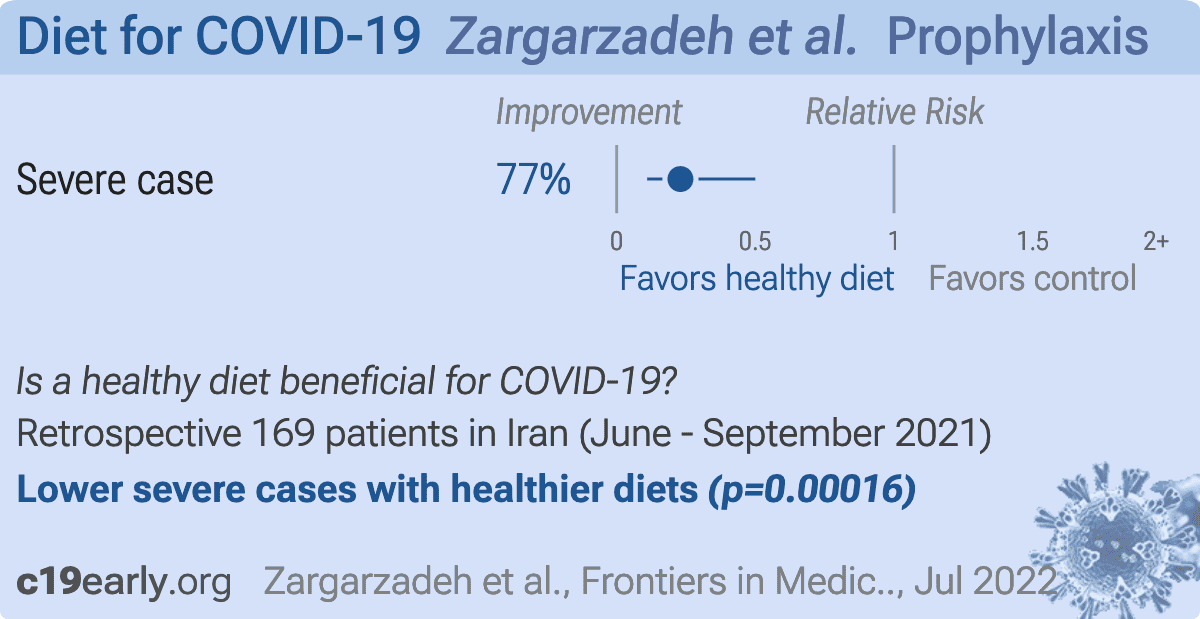
Zargarzadeh:
Retrospective 250 COVID-19 patients in Iran, showing lower risk of severe disease with greater adherence to a Mediterranean diet.
{kind=link}
Zhao:
UK Biobank retrospective 196,154 participants with 11,288 COVID-19 cases, showing lower COVID-19 mortality, severity, and incidence for lower dietary inflammatory scores.
{kind=link}
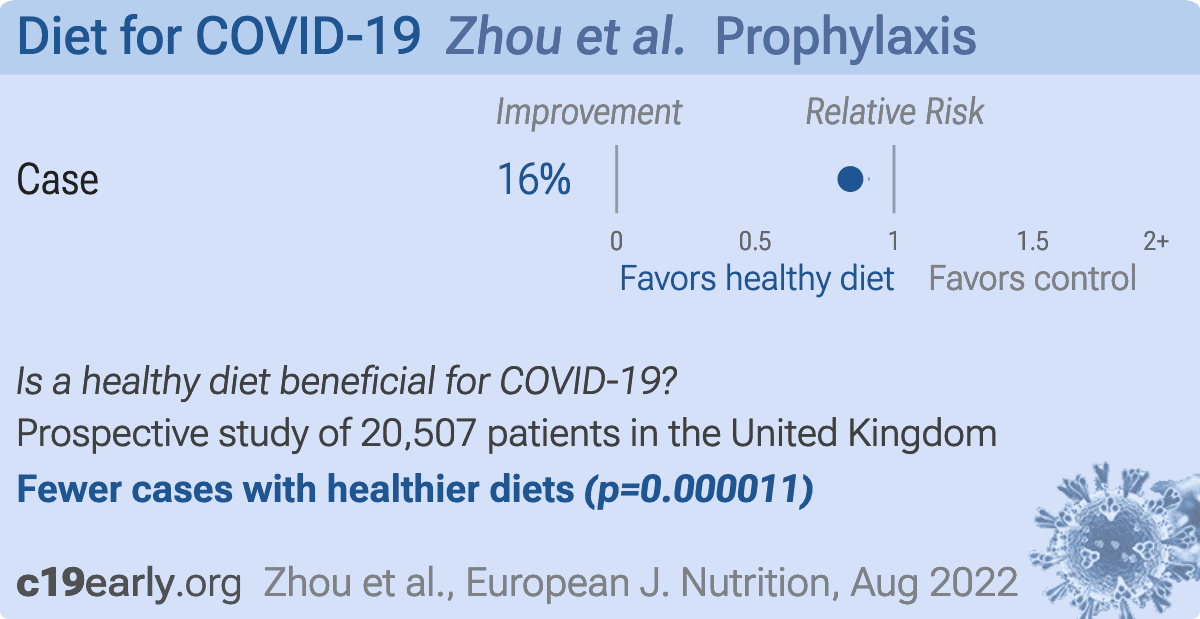
Zhou:
Prospective study of 41,012 UK Biobank participants, showing higher risk of COVID-19 cases with ultra-processed food consumption.
We perform ongoing searches of PubMed, medRxiv, Europe PMC,
ClinicalTrials.gov, The Cochrane Library, Google Scholar, Research
Square, ScienceDirect, Oxford University Press, the reference lists of other
studies and meta-analyses, and submissions to the site c19early.org.
Search terms are diet AND COVID-19. Automated searches are performed twice daily, with all matches reviewed for inclusion.
All studies regarding the use of diet for COVID-19 that report
a comparison with a control group are included in the main analysis.
Sensitivity analysis is performed, excluding studies with major issues,
epidemiological studies, and studies with minimal available information.
This is a living analysis and is updated regularly.
We extracted effect sizes and associated data from all studies.
If studies report multiple kinds of effects then the most serious
outcome is used in pooled analysis, while other outcomes are included in the
outcome specific analyses. For example, if effects for mortality and cases are
both reported, the effect for mortality is used, this may be different to the
effect that a study focused on.
If symptomatic
results are reported at multiple times, we used the latest time, for example
if mortality results are provided at 14 days and 28 days, the results at 28
days have preference. Mortality alone is preferred over combined outcomes.
Outcomes with zero events in both arms are not used, the next most serious
outcome with one or more events is used. For example, in low-risk populations
with no mortality, a reduction in mortality with treatment is not possible,
however a reduction in hospitalization, for example, is still valuable.
Clinical outcomes are considered more important than viral test status. When
basically all patients recover in both treatment and control groups,
preference for viral clearance and recovery is given to results mid-recovery
where available. After most or all patients have recovered there is little or
no room for an effective treatment to do better, however faster recovery is
valuable.
If only individual symptom data is available, the most serious symptom has
priority, for example difficulty breathing or low SpO2 is more
important than cough.
When results provide an odds ratio, we compute the relative risk when
possible, or convert to a relative risk according to Zhang.
Reported confidence intervals and p-values were used when available,
using adjusted values when provided. If multiple types of adjustments are
reported propensity score matching and multivariable regression has preference
over propensity score matching or weighting, which has preference over
multivariable regression. Adjusted results have preference over unadjusted
results for a more serious outcome when the adjustments significantly alter
results. When needed, conversion between reported p-values and
confidence intervals followed Altman, Altman (B), and Fisher's exact
test was used to calculate p-values for event data. If continuity
correction for zero values is required, we use the reciprocal of the opposite
arm with the sum of the correction factors equal to 1 Sweeting.
Results are expressed with RR < 1.0 favoring treatment, and using the risk of
a negative outcome when applicable (for example, the risk of death rather than
the risk of survival). If studies only report relative continuous values such
as relative times, the ratio of the time for the treatment group versus the
time for the control group is used. Calculations are done in Python
(3.12.3) with
scipy (1.13.0), pythonmeta (1.26), numpy (1.26.4), statsmodels (0.14.2), and plotly (5.21.0).
Forest plots are computed using PythonMeta Deng
with the DerSimonian and Laird random effects model (the fixed effect
assumption is not plausible in this case) and inverse variance weighting.
Results are presented with 95% confidence intervals. Heterogeneity among studies was
assessed using the I2 statistic.
Mixed-effects meta-regression results are computed with R (4.1.2) using the metafor
(3.0-2) and rms (6.2-0) packages, and using the most serious sufficiently powered outcome.
For all statistical tests, a p-value less than 0.05 was considered statistically significant.
Grobid 0.8.0 is used to parse PDF documents.
We have classified studies as early treatment if most patients
are not already at a severe stage at the time of treatment (for example based
on oxygen status or lung involvement), and treatment started within 5 days of
the onset of symptoms. If studies contain a mix of early treatment and late
treatment patients, we consider the treatment time of patients contributing
most to the events (for example, consider a study where most patients are
treated early but late treatment patients are included, and all mortality
events were observed with late treatment patients).
We note that a shorter time may be preferable. Antivirals are typically only
considered effective when used within a shorter timeframe, for example 0-36 or
0-48 hours for oseltamivir, with longer delays not being effective
McLean, Treanor.
We received no funding, this research is done in our spare
time. We have no affiliations with any pharmaceutical companies or political
parties.
A summary of study results is below. Please submit
updates and corrections at https://c19early.org/dtmeta.html.
Effect extraction follows pre-specified rules as detailed above
and gives priority to more serious outcomes.
For pooled analyses, the first (most serious) outcome is used, which may
differ from the effect a paper focuses on.
Other outcomes are used in outcome specific analyses.
| Tomasa-Irriguible, 11/30/2023, Double Blind Randomized Controlled Trial, placebo-controlled, Spain, trial NCT04751669 (history) (CoVIT). | Estimated 300 patient RCT with results unknown and over 4 months late. |
Effect extraction follows pre-specified rules as detailed above
and gives priority to more serious outcomes.
For pooled analyses, the first (most serious) outcome is used, which may
differ from the effect a paper focuses on.
Other outcomes are used in outcome specific analyses.
| Aghajani, 7/6/2023, retrospective, Iran, peer-reviewed, 4 authors, study period April 2022 - August 2022. | risk of severe case, 88.0% lower, OR 0.12, p < 0.001, higher quality diet 96, lower quality diet 85, adjusted per study, case control OR, DAQS tertile 3 vs. tertile 1, multivariable, model 3. |
| Ahmadi, 8/31/2021, retrospective, United Kingdom, peer-reviewed, 5 authors. | risk of death, 3.0% higher, RR 1.03, p = 0.85, adjusted per study, good vs. poor, model 2, multivariable. |
| Barania Adabi, 3/31/2023, retrospective, Iran, peer-reviewed, survey, mean age 40.3, 5 authors, study period March 2021 - September 2021. | risk of ICU admission, 98.7% lower, RR 0.01, p < 0.001, higher quality diet 0 of 125 (0.0%), lower quality diet 37 of 125 (29.6%), NNT 3.4, relative risk is not 0 because of continuity correction due to zero events (with reciprocal of the contrasting arm), DII, quartile I vs. quartile IV. |
| risk of ICU admission, 98.1% lower, RR 0.02, p < 0.001, higher quality diet 0 of 125 (0.0%), lower quality diet 26 of 125 (20.8%), NNT 4.8, relative risk is not 0 because of continuity correction due to zero events (with reciprocal of the contrasting arm), E-DII, quartile I vs. quartile IV. | |
| Ebrahimzadeh, 8/19/2022, retrospective, Iran, peer-reviewed, survey, 3 authors, study period June 2021 - September 2021. | risk of severe case, 69.0% lower, OR 0.31, p = 0.004, healthy diet, T3 vs. T1, model 3, RR approximated with OR. |
| risk of hospitalization, 56.0% lower, OR 0.44, p = 0.07, hospitalization time, healthy diet, T3 vs. T1, model 3, RR approximated with OR. | |
| risk of no recovery, 68.0% lower, OR 0.32, p = 0.003, recovery duration, healthy diet, T3 vs. T1, model 3, RR approximated with OR. | |
| Firoozi, 3/29/2022, retrospective, Iran, peer-reviewed, survey, 8 authors, study period March 2020 - June 2020. | risk of case, 65.0% lower, OR 0.35, p < 0.001, adjusted per study, inverted to make OR<1 favor higher quality diet, case control OR, multivariable, per unit E-DII change. |
| Hou, 4/29/2022, retrospective, Taiwan, peer-reviewed, survey, 3 authors, study period May 2021 - August 2021. | risk of critical case, 71.6% lower, RR 0.28, p = 0.23, higher quality diet 1 of 22 (4.5%), lower quality diet 78 of 487 (16.0%), NNT 8.7, excluded in exclusion analyses: unadjusted results with no group details. |
| risk of moderate to critical case, 10.8% lower, RR 0.89, p = 0.66, higher quality diet 11 of 22 (50.0%), lower quality diet 273 of 487 (56.1%), NNT 17, excluded in exclusion analyses: unadjusted results with no group details. | |
| risk of critical case, 73.6% lower, RR 0.26, p = 0.005, higher quality diet 0 of 9 (0.0%), lower quality diet 47 of 127 (37.0%), NNT 2.7, adjusted per study, inverted to make RR<1 favor higher quality diet, odds ratio converted to relative risk, multivariable, age >65. | |
| risk of moderate to critical case, 34.7% lower, RR 0.65, p = 0.04, higher quality diet 5 of 9 (55.6%), lower quality diet 108 of 127 (85.0%), NNT 3.4, age >65, excluded in exclusion analyses: unadjusted results with no group details. | |
| Jagielski, 1/14/2022, retrospective, Poland, peer-reviewed, 7 authors. | risk of case, 81.5% lower, RR 0.18, p = 0.005, higher quality diet 4 of 40 (10.0%), lower quality diet 9 of 20 (45.0%), NNT 2.9, adjusted per study, inverted to make RR<1 favor higher quality diet, odds ratio converted to relative risk, model 2, FV ≥ 500g and nuts ≥ 10g vs. FV < 500g and nuts < 10g, multivariable. |
| Kim, 6/7/2021, retrospective, multiple countries, peer-reviewed, survey, 8 authors, study period 17 July, 2020 - 25 September, 2020. | risk of moderate/severe case, 72.0% lower, OR 0.28, p = 0.02, higher quality diet 41, lower quality diet 527, adjusted per study, plant-based diets, multivariable, RR approximated with OR. |
| risk of moderate/severe case, 59.0% lower, OR 0.41, p = 0.05, higher quality diet 46, lower quality diet 522, adjusted per study, plant-based or pescatarian diets, multivariable, RR approximated with OR. | |
| risk of case, 19.0% lower, OR 0.81, p = 0.24, higher quality diet 41, lower quality diet 527, adjusted per study, plant-based diets, multivariable, RR approximated with OR. | |
| risk of case, 23.0% lower, OR 0.77, p = 0.14, higher quality diet 46, lower quality diet 522, adjusted per study, plant-based or pescatarian diets, multivariable, RR approximated with OR. | |
| Magaña, 12/31/2021, retrospective, Spain, peer-reviewed, 6 authors, excluded in exclusion analyses: unadjusted results with no group details. | risk of death, 53.0% lower, HR 0.47, p = 0.049, higher quality diet 58, lower quality diet 31. |
| Mahto, 2/15/2021, retrospective, India, peer-reviewed, 6 authors, excluded in exclusion analyses: unadjusted results with no group details. | risk of IgG positive, 20.4% lower, RR 0.80, p = 0.32, higher quality diet 23 of 206 (11.2%), lower quality diet 70 of 483 (14.5%), NNT 30, unadjusted, inverted to make RR<1 favor higher quality diet, odds ratio converted to relative risk. |
| Merino, 6/25/2021, retrospective, multiple countries, peer-reviewed, survey, 30 authors, study period 24 March, 2020 - 2 December, 2020. | risk of severe case, 41.0% lower, HR 0.59, p < 0.001, higher quality diet 148,142, lower quality diet 148,143, adjusted per study, model 3, high vs. low hPDI, multivariable, Cox proportional hazards. |
| risk of case, 18.0% lower, HR 0.82, p < 0.001, higher quality diet 148,142, lower quality diet 148,143, adjusted per study, model 3, high vs. low hPDI, PCR+, multivariable, Cox proportional hazards. | |
| risk of case, 9.0% lower, HR 0.91, p < 0.001, higher quality diet 148,142, lower quality diet 148,143, adjusted per study, model 3, high vs. low hPDI, multivariable, Cox proportional hazards. | |
| Micek, 8/3/2023, retrospective, Poland, peer-reviewed, survey, 8 authors, study period July 2020 - December 2020. | risk of case, 70.0% lower, OR 0.30, p = 0.09, higher quality diet 32, lower quality diet 21, adjusted per study, total polyphenols, T3 vs. T1, multivariable, RR approximated with OR. |
| Mohajeri, 1/26/2023, retrospective, Iran, peer-reviewed, survey, 3 authors, excluded in exclusion analyses: unadjusted results with no group details. | risk of progression, 25.4% lower, RR 0.75, p < 0.001, higher quality diet 62 of 105 (59.0%), lower quality diet 392 of 495 (79.2%), NNT 5.0, dyspnea. |
| risk of progression, 51.1% lower, RR 0.49, p < 0.001, higher quality diet 50 of 105 (47.6%), lower quality diet 482 of 495 (97.4%), NNT 2.0, fever. | |
| risk of progression, 70.3% lower, RR 0.30, p < 0.001, higher quality diet 23 of 105 (21.9%), lower quality diet 365 of 495 (73.7%), NNT 1.9, taste/smell. | |
| risk of progression, 9.7% higher, RR 1.10, p = 0.03, higher quality diet 98 of 105 (93.3%), lower quality diet 421 of 495 (85.1%), fatigue. | |
| risk of progression, 52.9% lower, RR 0.47, p < 0.001, higher quality diet 38 of 105 (36.2%), lower quality diet 380 of 495 (76.8%), NNT 2.5, cough. | |
| risk of progression, 25.9% lower, RR 0.74, p = 0.007, higher quality diet 44 of 105 (41.9%), lower quality diet 280 of 495 (56.6%), NNT 6.8, diarrhea. | |
| Moludi, 8/23/2021, retrospective, Iran, peer-reviewed, 7 authors, study period June 2020 - July 2020. | risk of case, 91.6% lower, OR 0.08, p < 0.001, inverted to make OR<1 favor higher quality diet, case control OR, model 3, E-DII tertile 1 vs. tertile 3. |
| Naushin, 4/20/2021, retrospective, India, peer-reviewed, survey, 136 authors. | risk of seropositive, 40.1% lower, OR 0.60, p < 0.001, inverted to make OR<1 favor higher quality diet, RR approximated with OR. |
| Nguyen, 9/18/2021, retrospective, Vietnam, peer-reviewed, survey, 17 authors, study period 14 February, 2020 - 2 March, 2020. | risk of symptomatic case, 15.2% lower, RR 0.85, p = 0.006, higher quality diet 345 of 1,054 (32.7%), lower quality diet 433 of 1,082 (40.0%), NNT 14, adjusted per study, odds ratio converted to relative risk, high vs. low HES, COVID-19-like symptoms, multivariable. |
| Pavlidou, 11/9/2023, retrospective, Greece, peer-reviewed, 14 authors. | risk of case, 55.0% lower, OR 0.45, p < 0.001, higher quality diet 2,609, lower quality diet 2,588, adjusted per study, inverted to make OR<1 favor higher quality diet, moderate/high vs. very low/low Mediterranean diet adherence, multivariable, RR approximated with OR. |
| Perez-Araluce, 1/24/2022, retrospective, Spain, peer-reviewed, survey, 4 authors, study period March 2020 - December 2020. | risk of severe case, 77.9% lower, RR 0.22, p = 0.15, higher quality diet 1 of 1,103 (0.1%), lower quality diet 10 of 3,300 (0.3%), NNT 471, odds ratio converted to relative risk, high vs. low adherence. |
| risk of symptomatic case, 15.1% lower, RR 0.85, p = 0.31, higher quality diet 52 of 1,103 (4.7%), lower quality diet 214 of 3,300 (6.5%), odds ratio converted to relative risk, high vs. low adherence. | |
| risk of case, 19.7% lower, RR 0.80, p = 0.14, higher quality diet 58 of 1,103 (5.3%), lower quality diet 248 of 3,300 (7.5%), odds ratio converted to relative risk, high vs. low adherence. | |
| Reis, 10/24/2022, retrospective, USA, peer-reviewed, survey, 6 authors, study period December 2020 - February 2021. | risk of hospitalization, 74.8% lower, RR 0.25, p < 0.001, higher quality diet 17 of 380 (4.5%), lower quality diet 21 of 166 (12.7%), adjusted per study, inverted to make RR<1 favor higher quality diet, odds ratio converted to relative risk, 3+ vegetable servings/day vs. <3, multivariable. |
| Tadbir Vajargah, 9/29/2022, prospective, Iran, peer-reviewed, survey, mean age 44.2, 11 authors, study period June 2021 - September 2021. | risk of severe case, 67.0% lower, OR 0.33, p = 0.003, higher quality diet 83, lower quality diet 83, vegetables, highest vs. lowest tertile, RR approximated with OR. |
| risk of severe case, 72.0% lower, OR 0.28, p < 0.001, higher quality diet 83, lower quality diet 83, fruit, highest vs. lowest tertile, RR approximated with OR. | |
| risk of severe case, 75.0% lower, OR 0.25, p < 0.001, higher quality diet 83, lower quality diet 83, fiber, highest vs. lowest tertile, RR approximated with OR. | |
| Wang, 7/31/2023, retrospective, China, peer-reviewed, 9 authors, study period April 2022 - June 2022. | risk of severe case, 45.0% lower, OR 0.55, p = 0.06, higher quality diet 81, lower quality diet 67, adjusted per study, MNA-SF >11 vs. ≤11, multivariable, RR approximated with OR. |
| risk of no viral clearance, 31.5% lower, HR 0.68, p = 0.03, higher quality diet 81, lower quality diet 67, inverted to make HR<1 favor higher quality diet, MNA-SF >11 vs. ≤11, Cox proportional hazards. | |
| Wang (B), 2/6/2023, prospective, USA, peer-reviewed, survey, mean age 64.7, 8 authors, study period April 2020 - November 2021. | risk of PASC, 9.0% lower, RR 0.91, p = 0.43, higher quality diet 124 of 318 (39.0%), lower quality diet 218 of 480 (45.4%), NNT 16, adjusted per study, Q5 vs. Q1, multivariable, model 2. |
| risk of PASC, 49.0% lower, RR 0.51, p = 0.002, higher quality diet 188, lower quality diet 66, 5 or 6 healthy lifestyle factors vs. 0. | |
| Yamamoto, 12/30/2021, retrospective, USA, peer-reviewed, survey, mean age 35.0, 3 authors, excluded in exclusion analyses: unadjusted results with no group details. | risk of case, 66.3% lower, RR 0.34, p = 0.009, higher quality diet 4 of 20 (20.0%), lower quality diet 19 of 32 (59.4%), NNT 2.5, good, very good, excellent vs. fair, poor. |
| Yue, 8/9/2022, retrospective, multiple countries, peer-reviewed, survey, 11 authors. | risk of case, 19.0% lower, OR 0.81, p = 0.008, Q4 vs. Q1, model 3 + IPW, AHEI, RR approximated with OR. |
| risk of case, 21.0% lower, OR 0.79, p = 0.006, Q4 vs. Q1, model 3 + IPW, AMED, RR approximated with OR. | |
| risk of case, 28.6% lower, OR 0.71, p < 0.001, inverted to make OR<1 favor higher quality diet, Q1 vs. Q4, model 3 + IPW, EDIH, RR approximated with OR. | |
| risk of case, 11.5% lower, OR 0.88, p = 0.10, inverted to make OR<1 favor higher quality diet, Q1 vs. Q4, model 3 + IPW, EDIP, RR approximated with OR. | |
| Zamanian, 3/3/2023, retrospective, Iran, peer-reviewed, mean age 46.2, 10 authors. | risk of hospitalization, 81.0% lower, OR 0.19, p = 0.002, higher quality diet 41, lower quality diet 53, adjusted per study, case control OR, DASH ≥27 vs. ≤22, multivariable, model 3. |
| Zargarzadeh, 7/19/2022, retrospective, Iran, peer-reviewed, mean age 44.1, 11 authors, study period June 2021 - September 2021. | risk of severe case, 77.0% lower, OR 0.23, p < 0.001, higher quality diet 89, lower quality diet 80, adjusted per study, top tertile vs. lowest tertile, MD score, model 3, multivariable, RR approximated with OR. |
| Zhao, 12/14/2022, retrospective, United Kingdom, peer-reviewed, survey, 9 authors, study period January 2020 - March 2021. | risk of death, 24.2% lower, RR 0.76, p = 0.13, higher quality diet 39,230, lower quality diet 39,231, adjusted per study, inverted to make RR<1 favor higher quality diet, E-DII, quintile 1 vs. quintile 5, multivariable, model 4. |
| risk of death, 30.1% lower, RR 0.70, p = 0.04, higher quality diet 39,230, lower quality diet 39,231, adjusted per study, inverted to make RR<1 favor higher quality diet, DII, quintile 1 vs. quintile 5, multivariable, model 4. | |
| risk of severe case, 28.1% lower, RR 0.72, p < 0.001, higher quality diet 39,230, lower quality diet 39,231, adjusted per study, inverted to make RR<1 favor higher quality diet, E-DII, quintile 1 vs. quintile 5, multivariable, model 4. | |
| risk of severe case, 28.6% lower, RR 0.71, p < 0.001, higher quality diet 39,230, lower quality diet 39,231, adjusted per study, inverted to make RR<1 favor higher quality diet, DII, quintile 1 vs. quintile 5, multivariable, model 4. | |
| risk of case, 14.5% lower, RR 0.85, p < 0.001, higher quality diet 39,230, lower quality diet 39,231, adjusted per study, inverted to make RR<1 favor higher quality diet, E-DII, quintile 1 vs. quintile 5, multivariable, model 4. | |
| risk of case, 9.1% lower, RR 0.91, p = 0.002, higher quality diet 39,230, lower quality diet 39,231, adjusted per study, inverted to make RR<1 favor higher quality diet, DII, quintile 1 vs. quintile 5, multivariable, model 4. | |
| Zhou, 8/16/2022, prospective, United Kingdom, peer-reviewed, 6 authors. | risk of case, 15.7% lower, RR 0.84, p < 0.001, higher quality diet 1,321 of 10,254 (12.9%), lower quality diet 1,935 of 10,253 (18.9%), inverted to make RR<1 favor higher quality diet, odds ratio converted to relative risk, Q4 vs. Q1, model 3 (before healthy diet score adjustment). |
Aghajani et al., Association between dietary antioxidant quality score and severity of coronavirus infection: a case–control study, Frontiers in Nutrition, doi:10.3389/fnut.2023.1174113.
Ahmadi et al., Lifestyle risk factors and infectious disease mortality, including COVID-19, among middle aged and older adults: Evidence from a community-based cohort study in the United Kingdom, Brain, Behavior, and Immunity, doi:10.1016/j.bbi.2021.04.022.
Altman (B) et al., How to obtain the confidence interval from a P value, BMJ, doi:10.1136/bmj.d2090.
Barania Adabi et al., The association between inflammatory and immune system biomarkers and the dietary inflammatory index in patients with COVID-19, Frontiers in Nutrition, doi:10.3389/fnut.2023.1075061.
Ebrahimzadeh et al., Major dietary patterns in relation to disease severity, symptoms, and inflammatory markers in patients recovered from COVID-19, Frontiers in Nutrition, doi:10.3389/fnut.2022.929384.
Firoozi et al., The Association between Energy-Adjusted Dietary Inflammatory Index, Body Composition, and Anthropometric Indices in COVID-19-Infected Patients: A Case-Control Study in Shiraz, Iran, International Journal of Clinical Practice, doi:10.1155/2022/5452488.
Hao et al., Association of dietary inflammatory index and the SARS-CoV-2 infection incidence, severity and mortality of COVID-19: a systematic review and dose-response meta-analysis, Nutrition Journal, doi:10.1186/s12937-024-00927-3.
Hou et al., COVID-19 Illness Severity in the Elderly in Relation to Vegetarian and Non-vegetarian Diets: A Single-Center Experience, Frontiers in Nutrition, doi:10.3389/fnut.2022.837458.
Jagielski et al., Associations of Nutritional Behavior and Gut Microbiota with the Risk of COVID-19 in Healthy Young Adults in Poland, Nutrients, doi:10.3390/nu14020350.
Kahleova et al., The Role of Nutrition in COVID-19: Taking a Lesson from the 1918 H1N1 Pandemic, American Journal of Lifestyle Medicine, doi:10.1177/15598276221097621.
Kim et al., Plant-based diets, pescatarian diets and COVID-19 severity: a population-based case–control study in six countries, BMJ Nutrition, Prevention & Health, doi:10.1136/bmjnph-2021-000272.
Lui et al., Nsp1 facilitates SARS-CoV-2 replication through calcineurin-NFAT signaling, Virology, doi:10.1128/mbio.00392-24.
Lv et al., Host proviral and antiviral factors for SARS-CoV-2, Virus Genes, doi:10.1007/s11262-021-01869-2.
Magaña et al., Influence of mediterranean diet on survival from covid-19 disease, Clinical Nutrition ESPEN, doi:10.1016/j.clnesp.2021.09.606.
Mahto et al., Seroprevalence of IgG against SARS-CoV-2 and its determinants among healthcare workers of a COVID-19 dedicated hospital of India, American Journal of Blood Research, 11:1, www.ncbi.nlm.nih.gov/labs/pmc/articles/PMC8010601/.
Malone et al., Structures and functions of coronavirus replication–transcription complexes and their relevance for SARS-CoV-2 drug design, Nature Reviews Molecular Cell Biology, doi:10.1038/s41580-021-00432-z.
McLean et al., Impact of Late Oseltamivir Treatment on Influenza Symptoms in the Outpatient Setting: Results of a Randomized Trial, Open Forum Infect. Dis. September 2015, 2:3, doi:10.1093/ofid/ofv100.
Merino et al., Diet quality and risk and severity of COVID-19: a prospective cohort study, Gut, doi:10.1136/gutjnl-2021-325353.
Micek et al., Association of dietary intake of polyphenols, lignans, and phytosterols with immune-stimulating microbiota and COVID-19 risk in a group of Polish men and women, Frontiers in Nutrition, doi:10.3389/fnut.2023.1241016.
Mohajeri et al., Adherence to the Mediterranean Diet Association with Serum Inflammatory Factors Stress Oxidative and Appetite in COVID-19 Patients, Medicina, doi:10.3390/medicina59020227.
Moludi et al., The relationship between Dietary Inflammatory Index and disease severity and inflammatory status: a case–control study of COVID-19 patients, British Journal of Nutrition, doi:10.1017/S0007114521003214.
Murigneux et al., Proteomic analysis of SARS-CoV-2 particles unveils a key role of G3BP proteins in viral assembly, Nature Communications, doi:10.1038/s41467-024-44958-0.
Naushin et al., Insights from a Pan India Sero-Epidemiological survey (Phenome-India Cohort) for SARS-CoV2, eLife, doi:10.7554/eLife.66537.
Nguyen et al., Single and Combinative Impacts of Healthy Eating Behavior and Physical Activity on COVID-19-like Symptoms among Outpatients: A Multi-Hospital and Health Center Survey, Nutrients, doi:10.3390/nu13093258.
Niarakis et al., Drug-target identification in COVID-19 disease mechanisms using computational systems biology approaches, Frontiers in Immunology, doi:10.3389/fimmu.2023.1282859.
Pavlidou et al., Association of COVID-19 Infection with Sociodemographic, Anthropometric and Lifestyle Factors: A Cross-Sectional Study in an Older Adults’ Population Aged over 65 Years Old, Diseases, doi:10.3390/diseases11040165.
Perez-Araluce et al., Components of the Mediterranean Diet and Risk of COVID-19, Frontiers in Nutrition, doi:10.3389/fnut.2021.805533.
Rahmati et al., The effect of adherence to high-quality dietary pattern on COVID-19 outcomes: A systematic review and meta-analysis, Journal of Medical Virology, doi:10.1002/jmv.28298.
Reis et al., The Association between Lifestyle Risk Factors and COVID-19 Hospitalization in a Healthcare Institution, American Journal of Lifestyle Medicine, doi:10.1177/15598276221135541.
Singh et al., The relationship between viral clearance rates and disease progression in early symptomatic COVID-19: a systematic review and meta-regression analysis, Journal of Antimicrobial Chemotherapy, doi:10.1093/jac/dkae045.
Sweeting et al., What to add to nothing? Use and avoidance of continuity corrections in meta-analysis of sparse data, Statistics in Medicine, doi:10.1002/sim.1761.
Tadbir Vajargah et al., Association of fruits, vegetables, and fiber intake with COVID-19 severity and symptoms in hospitalized patients: A cross-sectional study, Frontiers in Nutrition, doi:10.3389/fnut.2022.934568.
Tomasa-Irriguible et al., Efficacy of Micronutrient Dietary Supplementation in Reducing Hospital Admissions for COVID-19: A Double-blind, Placebo-controlled, Randomized Clinical Trial, NCT04751669, clinicaltrials.gov/study/NCT04751669.
Treanor et al., Efficacy and Safety of the Oral Neuraminidase Inhibitor Oseltamivir in Treating Acute Influenza: A Randomized Controlled Trial, JAMA, 2000, 283:8, 1016-1024, doi:10.1001/jama.283.8.1016.
Wang et al., Improving Nutritional Status Was Associated with Decreasing Disease Severity and Shortening of Negative Conversion Time of PCR Test in Non-ICU Patients with COVID-19, Infection and Drug Resistance, doi:10.2147/idr.s409615.
Wang (B) et al., Adherence to Healthy Lifestyle Prior to Infection and Risk of Post–COVID-19 Condition, JAMA Internal Medicine, doi:10.1001/jamainternmed.2022.6555.
Yamamoto et al., Flight attendant occupational nutrition and lifestyle factors associated with COVID-19 incidence, Scientific Reports, doi:10.1038/s41598-021-04350-0.
Yue et al., Long-term diet and risk of SARS -CoV-2 infection and Coronavirus Disease 2019 (COVID-19) severity, The American Journal of Clinical Nutrition, doi:10.1093/ajcn/nqac219.
Zamanian et al., The association of dietary approach to stop hypertension (DASH) diet with hospitalization risk in patients with COVID-19, Clinical Nutrition Open Science, doi:10.1016/j.nutos.2023.02.001.
Zargarzadeh et al., Higher Adherence to the Mediterranean Dietary Pattern Is Inversely Associated With Severity of COVID-19 and Related Symptoms: A Cross-Sectional Study, Frontiers in Medicine, doi:10.3389/fmed.2022.911273.
Zhang et al., What's the relative risk? A method of correcting the odds ratio in cohort studies of common outcomes, JAMA, 80:19, 1690, doi:10.1001/jama.280.19.1690.
Please send us corrections, updates, or comments.
c19early involves the extraction of 100,000+ datapoints from
thousands of papers. Community updates
help ensure high accuracy.
Treatments and other interventions are complementary.
All practical, effective, and safe
means should be used based on risk/benefit analysis.
No treatment or intervention is 100% available and effective for all current
and future variants.
We do not provide medical advice. Before taking any medication,
consult a qualified physician who can provide personalized advice and details
of risks and benefits based on your medical history and situation. FLCCC and WCH
provide treatment protocols.