Nirmatrelvir Plus Ritonavir for Early COVID-19 in a Large U.S. Health System
MD, MSc Scott Dryden-Peterson, BS Andy Kim, MD Arthur Y Kim, ScD Ellen C Caniglia, MD, MPH, MBA Inga T Lennes, MD, MPH Rajesh Patel, RN Lindsay Gainer, RN Lisa Dutton, RN, MSN, NP-C Elizabeth Donahue, MD Rajesh T Gandhi, MD Lindsey R Baden, MD, MPH Ann E Woolley
Annals of Internal Medicine, doi:10.7326/m22-2141
Background: In the EPIC-HR (Evaluation of Protease Inhibition for Covid-19 in High-Risk Patients) trial, nirmatrelvir plus ritonavir led to an 89% reduction in hospitalization or death among unvaccinated outpatients with early COVID-19. The clinical impact of nirmatrelvir plus ritonavir among vaccinated populations is uncertain. Objective: To assess whether nirmatrelvir plus ritonavir reduces risk for hospitalization or death among outpatients with early COVID-19 in the setting of prevalent SARS-CoV-2 immunity and immune-evasive SARS-CoV-2 lineages. Design: Population-based cohort study analyzed to emulate a clinical trial using inverse probability-weighted models to account for anticipated bias in treatment. Setting: A large health care system providing care for 1.5 million patients in Massachusetts and New Hampshire during the Omicron wave (1 January to 17 July 2022). Patients: 44 551 nonhospitalized adults (90.3% with ≥3 vaccine doses) aged 50 years or older with COVID-19 and no contraindications for nirmatrelvir plus ritonavir.
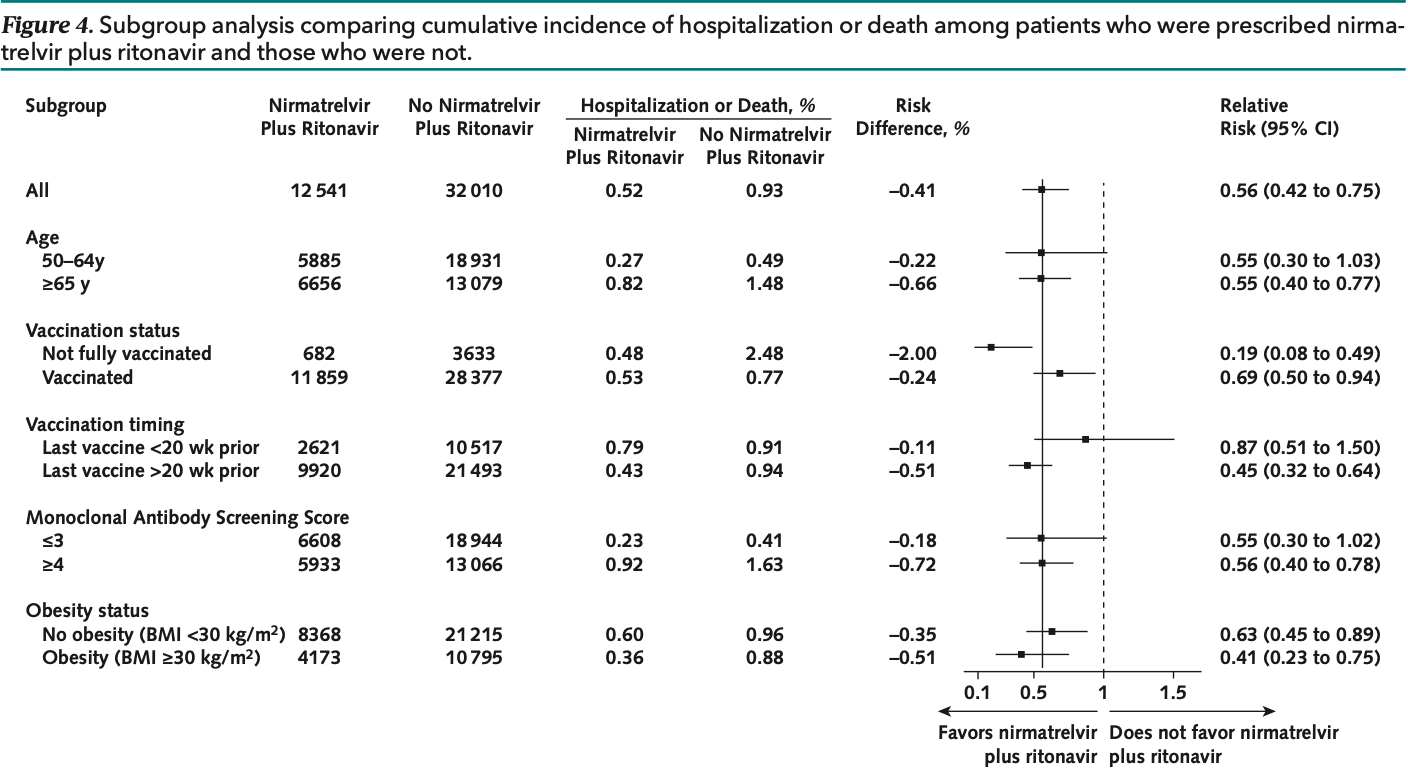
Measurements: The primary outcome was a composite of hospitalization within 14 days or death within 28 days of a COVID-19 diagnosis. Results: During the study period, 12 541 (28.1%) patients were prescribed nirmatrelvir plus ritonavir, and 32 010 (71.9%) were not. Patients prescribed nirmatrelvir plus ritonavir were more likely to be older, have more comorbidities, and be vaccinated. The composite outcome of hospitalization or death occurred in 69 (0.55%) patients who were prescribed nirmatrelvir plus ritonavir and 310 (0.97%) who were not (adjusted risk ratio, 0.56 [95% CI, 0.42 to 0.75]). Recipients of nirmatrelvir plus ritonavir had lower risk for hospitalization (adjusted risk ratio, 0.60 [CI, 0.44 to 0.81]) and death (adjusted risk ratio, 0.29 [CI, 0.12 to 0.71]). Limitation: Potential residual confounding due to differential access to COVID-19 vaccines, diagnostic tests, and treatment.
Conclusion: The overall risk for hospitalization or death was already low (1%) after an outpatient diagnosis of COVID-19, but nirmatrelvir plus ritonavir reduced this risk further.
Author contributions are available at Annals.org. Previous Posting: This manuscript was posted as a preprint on medRxiv on 17 June 2022. doi:10.1101/2022.06. 14.22276393
References
Administrative, Kim, Lennes, Patel, Gainer et al., logistic support
Arbel, Sagy, Hoshen, Nirmatrelvir use and severe Covid-19 outcomes during the Omicron surge, N Engl J Med,
doi:10.1056/NEJMoa2204919Bar-On, Goldberg, Mandel, Protection of BNT162b2 vaccine booster against Covid-19 in Israel, N Engl J Med,
doi:10.1056/NEJMoa2114255Cole, Hernán, Constructing inverse probability weights for marginal structural models, Am J Epidemiol,
doi:10.1093/aje/kwn164Denz, Klaaßen-Mielke, Timmesfeld, Boucau, Uddin et al., Virologic characterization of symptom rebound following nirmatrelvir-ritonavir treatment for COVID-19. medRxiv,
doi:10.1101/2022.05.24.22275326Dryden-Peterson, Kim, Caniglia, Patel, Dutton et al., ORIGINAL RESEARCH Nirmatrelvir Plus Ritonavir for Early COVID-19 in a Large U.S. Health System Author Contributions: Conception and design
Ganatra, Dani, Ahmad, Oral nirmatrelvir and ritonavir in non-hospitalized vaccinated patients with Covid-19, Clin Infect Dis,
doi:10.1093/cid/ciac673Ganesh, Philpot, Bierle, Real-world clinical outcomes of bamlanivimab and casirivimab-imdevimab among high-risk patients with mild to moderate coronavirus disease 2019, J Infect Dis,
doi:10.1093/infdis/jiab377Hammond, Leister-Tebbe, Gardner, EPIC-HR Investigators. Oral nirmatrelvir for high-risk, nonhospitalized adults with Covid-19, N Engl J Med,
doi:10.1056/NEJMoa2118542House, National COVID-19 Preparedness Plan
House, National COVID-19 Preparedness Plan
Kind, Jencks, Brock, Neighborhood socioeconomic disadvantage and 30-day rehospitalization: a retrospective cohort study, Ann Intern Med,
doi:10.7326/M13-2946Lambrou, Shirk, Steele, Genomic surveillance for SARS-CoV-2 variants: predominance of the Delta (B.1.617.2) and Omicron (B.1.1.529) variants-United States, MMWR Morb Mortal Wkly Rep,
doi:10.15585/mmwr.mm7106a4Liang, Zeger, Cole, Hernán, Longitudinal data analysis using generalized linear models, Comput Methods Programs Biomed,
doi:10.1093/biomet/73.1.13O'horo, Challener, Speicher, Effectiveness of monoclonal antibodies in preventing severe COVID-19 with emergence of the Delta variant, Mayo Clin Proc,
doi:10.1056/NEJMp1802313Zou, A modified Poisson regression approach to prospective studies with binary data, Am J Epidemiol



{kind=link}