Prior Glucose-Lowering Medication Use and 30-Day Outcomes Among 64,892 Veterans With Diabetes and COVID-19
Pandora L Wander, Elliott Lowy, Lauren A Beste, Luis Tulloch-Palomino, Anna Korpak, Alexander C Peterson, Steven E Kahn, Edward J Boyko
Diabetes Care, doi:10.2337/dc21-1351
To identify preinfection risk factors for adverse outcomes among veterans with diabetes and coronavirus disease 2019 (COVID-19) infection.
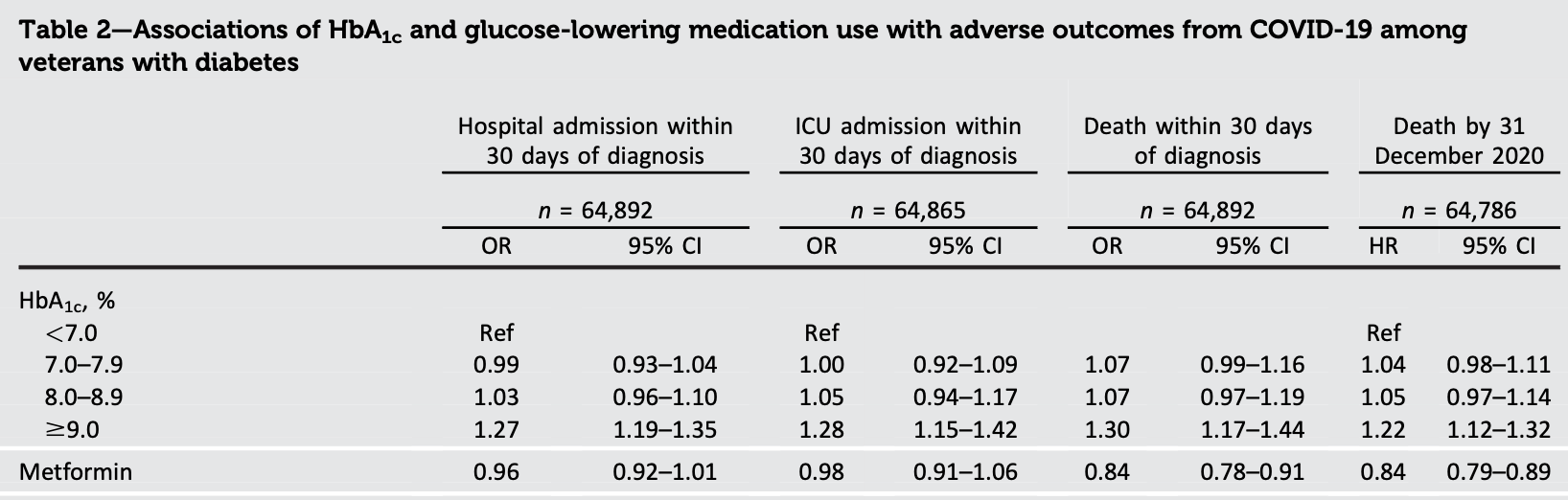
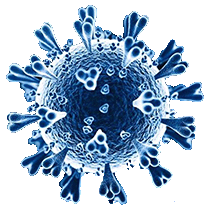
RESEARCH DESIGN AND METHODS We identified all Veterans Health Administration patients with diabetes and one or more positive nasal swab(s) for severe acute respiratory syndrome coronavirus 2 (1 March 2020-10 March 2021) (n = 64,892). We examined associations of HbA 1c and glucose-lowering medication use with hospitalization, intensive care unit (ICU) admission, and mortality at 30 days using logistic regression models and during 4.4 months of follow-up (range <1-13.1) using proportional hazards models.
RESULTS Compared with HbA 1c <7.0%, HbA 1c ‡9.0% was associated with higher odds of hospitalization, ICU admission, and death at 30 days (odds ratio [
Continued on p. 5 Author Contributions. P.L.W. conceived the project, designed the overall research plan, and wrote the first draft of the manuscript. E.L. analyzed the data and reviewed and edited the manuscript. L.A.B. reviewed and edited the manuscript. L.T.-P. reviewed and edited the manuscript. A.K. contributed to design and interpretation of the analyses and reviewed and edited the manuscript. A.C.P. contributed to the design and interpretation of the analyses and reviewed and edited the manuscript. S.E.K. contributed to the design of the analyses and reviewed and edited the manuscript. E.J.B. conceived the project, designed the overall research plan, and reviewed and edited the manuscript. P.L.W. and E.J.B. are the guarantors of this work and, as such, had full access to all the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis.
References
Apicella, Campopiano, Mantuano, Mazoni, Coppelli et al., COVID-19 in people with diabetes: understanding the reasons for worse outcomes, Lancet Diabetes Endocrinol
Bangi, Barve, Qamar, Protective effects of CVD and DM medications in SARS-CoV-2 Infection, SN Compr Clin Med
Dennis, Mcgovern, Vollmer, Mateen, Improving survival of critical care patients with coronavirus disease 2019 in England: a national cohort study, March to June 2020, Crit Care Med
Holman, Knighton, Kar, Risk factors for COVID-19-related mortality in people with type 1 and type 2 diabetes in England: a populationbased cohort study, Lancet Diabetes Endocrinol
Kahkoska, Abrahamsen, Alexander, N3C Consortium. Association between glucagon-like peptide 1 receptor agonist and sodium-glucose cotransporter 2 inhibitor use and COVID-19 Outcomes, Diabetes Care
Khunti, Knighton, Zaccardi, Prescription of glucose-lowering therapies and risk of COVID-19 mortality in people with type 2 diabetes: a nationwide observational study in England, Lancet Diabetes Endocrinol
Wander, Lowy, Beste, Risk factors for adverse outcomes among 35 879 veterans with and without diabetes after diagnosis with COVID-19, BMJ Open Diabetes Res Care

{kind=link}
{kind=link}