Association of Remdesivir Treatment With Survival and Length of Hospital Stay Among US Veterans Hospitalized With COVID-19
MD, MSPH Michael E Ohl, ScD Donald R Miller, PharmD Brian C Lund, MD Takaaki Kobayashi, PhD Kelly Richardson Miell, MA Brice F Beck, PharmD Bruce Alexander, MD Kristina Crothers, Mary S Vaughan Sarrazin
JAMA Network Open, doi:10.1001/jamanetworkopen.2021.14741
IMPORTANCE Randomized clinical trials have yielded conflicting results about the effects of remdesivir therapy on survival and length of hospital stay among people with COVID-19. OBJECTIVE To examine associations between remdesivir treatment and survival and length of hospital stay among people hospitalized with COVID-19 in routine care settings. DESIGN, SETTING, AND PARTICIPANTS This retrospective cohort study used data from the Veterans Health Administration (VHA) to identify adult patients in 123 VHA hospitals who had a first hospitalization with laboratory-confirmed COVID-19 from May 1 to October 8, 2020. Propensity score matching of patients initiating remdesivir treatment to control patients who had not initiated remdesivir treatment by the same hospital day was used to create the analytic cohort. EXPOSURES Remdesivir treatment. MAIN OUTCOMES AND MEASURES Time to death within 30 days of remdesivir treatment initiation (or corresponding hospital day for matched control individuals) and time to hospital discharge with time to death as a competing event. Associations between remdesivir treatment and these outcomes were assessed using Cox proportional hazards regression in the matched cohort.
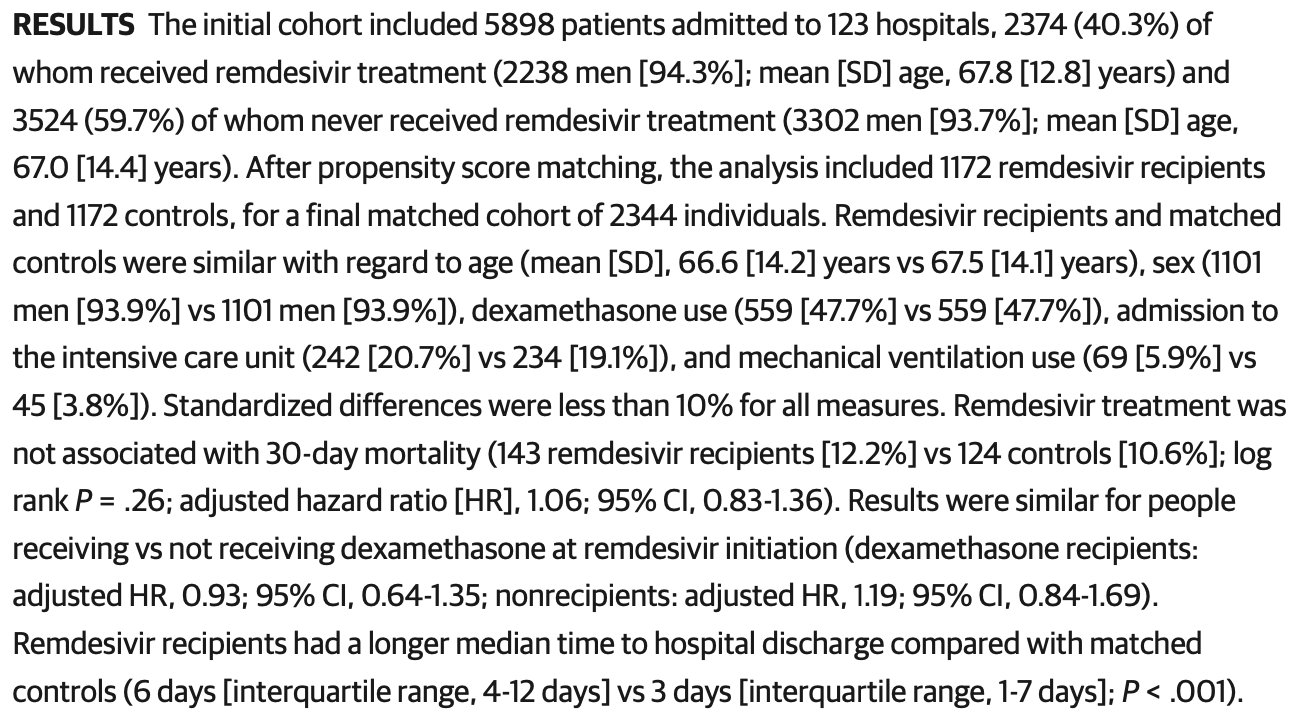
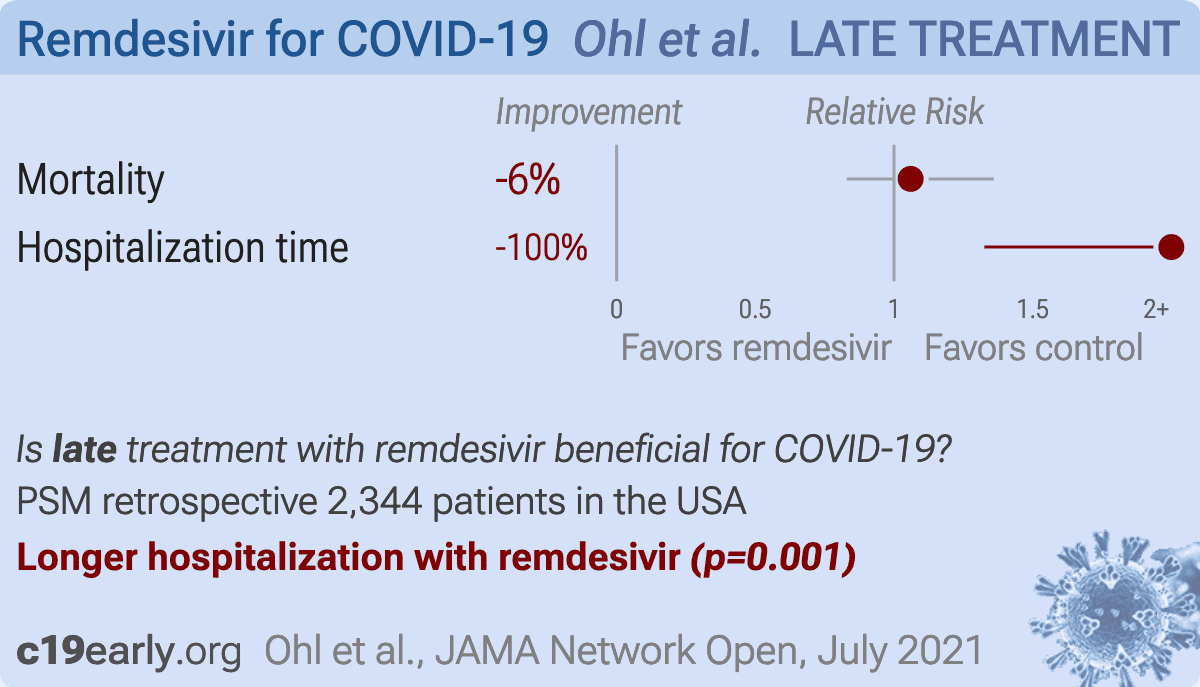
RESULTS The initial cohort included 5898 patients admitted to 123 hospitals, 2374 (40.3%) of whom received remdesivir treatment (2238 men [94.3%]; mean [SD] age, 67.8 [12.8] years) and 3524 (59.7%) of whom never received remdesivir treatment (3302 men [93.7%]; mean [SD] age, 67.0 [14.4] years). After propensity score matching, the analysis included 1172 remdesivir recipients and 1172 controls, for a final matched cohort of 2344 individuals. Remdesivir recipients and matched controls were similar with regard to age (mean [SD], 66.6 [14.2] years vs 67.5 [14.1] years), sex (1101 men [93.9%] vs 1101 men [93.9%]), dexamethasone use (559 [47.7%] vs 559 [47.7%]), admission to the intensive care unit (242 [20.7%] vs 234 [19.1%]), and mechanical ventilation use (69 [5.9%] vs 45 [3.8%]). Standardized differences were less than 10% for all measures. Remdesivir treatment was not associated with 30-day mortality (143 remdesivir recipients [12.2%] vs 124 controls [10.6%]; log rank P = .26; adjusted hazard ratio [HR], 1.06; 95% CI, 0.83-1.36). Results were similar for people receiving vs not receiving dexamethasone at remdesivir initiation (dexamethasone recipients:
be extrapolated to patients who do not resemble those in the propensity score-matched cohort. In addition, this study of US veterans included a small number of women, which affects the generalizability of the findings to the overall population. Third, limitations in available data prevented us from identifying specific subgroups of patients who may have been more likely to benefit from remdesivir treatment and from precisely emulating clinical trials. Subgroup analyses in the ACTT-1 suggested that remdesivir was most effective when patients required supplemental oxygen but had not yet progressed to require mechanical ventilation. 4 It is biologically plausible that remdesivir treatment is most beneficial during the early, viral replication phase of COVID-19, when antiviral drugs can still alter the course of illness before severe lung injury occurs. 3 Although we had data on oxygen saturation levels for patients during hospitalization and the matched remdesivir recipients and controls were balanced based on these values, we lacked data on the time from symptom onset to remdesivir initiation and the amount of supplemental oxygen patients required during hospitalization. We were therefore not able to examine variation in the outcomes associated with remdesivir according to phase of illness.
Conclusions In this cohort study of US veterans hospitalized with COVID-19, remdesivir treatment was not associated with survival but was associated with longer hospitalization. These..
References
Administrative, technical, or material support
Agostini, Andres, Sims, Coronavirus susceptibility to the antiviral remdesivir (GS-5734) is mediated by the viral polymerase and the proofreading exoribonuclease, mBio,
doi:10.1128/mBio.00221-18Austin, Balance diagnostics for comparing the distribution of baseline covariates between treatment groups in propensity-score matched samples, Stat Med,
doi:10.1002/sim.3697Beigel, Tomashek, Dodd, ACTT-1 Study Group Members. Remdesivir for the treatment of Covid-19-final report, N Engl J Med,
doi:10.1056/NEJMoa2007764Hernán, Brumback, Robins, Marginal structural models to estimate the causal effect of zidovudine on the survival of HIV-positive men, Epidemiology,
doi:10.1097/00001648-200009000-00012Horby, Lim, Emberson, Dexamethasone in hospitalized patients with COVID-19-preliminary report, N Engl J Med,
doi:10.1056/NEJMoa2021436Ohl, Kobayashi, Miell, Alexander, Sarrazin, Acquisition, analysis, or interpretation of data: All authors
Ohl, Md, Msph, None
Ohl, Sarrazin, the study and take responsibility for the integrity of the data and the accuracy of the data analysis
Pan, Peto, Henao-Restrepo, WHO Solidarity Trial Consortium. Repurposed antiviral drugs for Covid-19-interim WHO Solidarity Trial results, N Engl J Med,
doi:10.1056/NEJMoa2023184Rubin, Chan-Tack, Farley, Sherwat, FDA approval of remdesivir-a step in the right direction, N Engl J Med,
doi:10.1056/NEJMp2032369Von Elm, Altman, Egger, Pocock, Gøtzsche et al., The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies, Lancet,
doi:10.1016/S0140-6736(07)61602-XWang, Zhang, Du, Remdesivir in adults with severe COVID-19: a randomised, double-blind, placebocontrolled, multicentre trial, Lancet,
doi:10.1016/S0140-6736(20)31022-9


{kind=link}