HCQ for COVID-19
1st treatment shown to reduce risk in
March 2020
No treatment is 100% effective. Protocols
combine complementary and synergistic treatments. * >10%
efficacy in meta analysis with ≥3 clinical studies.
4,000+ studies for
60+ treatments. c19hcq.org
|
|
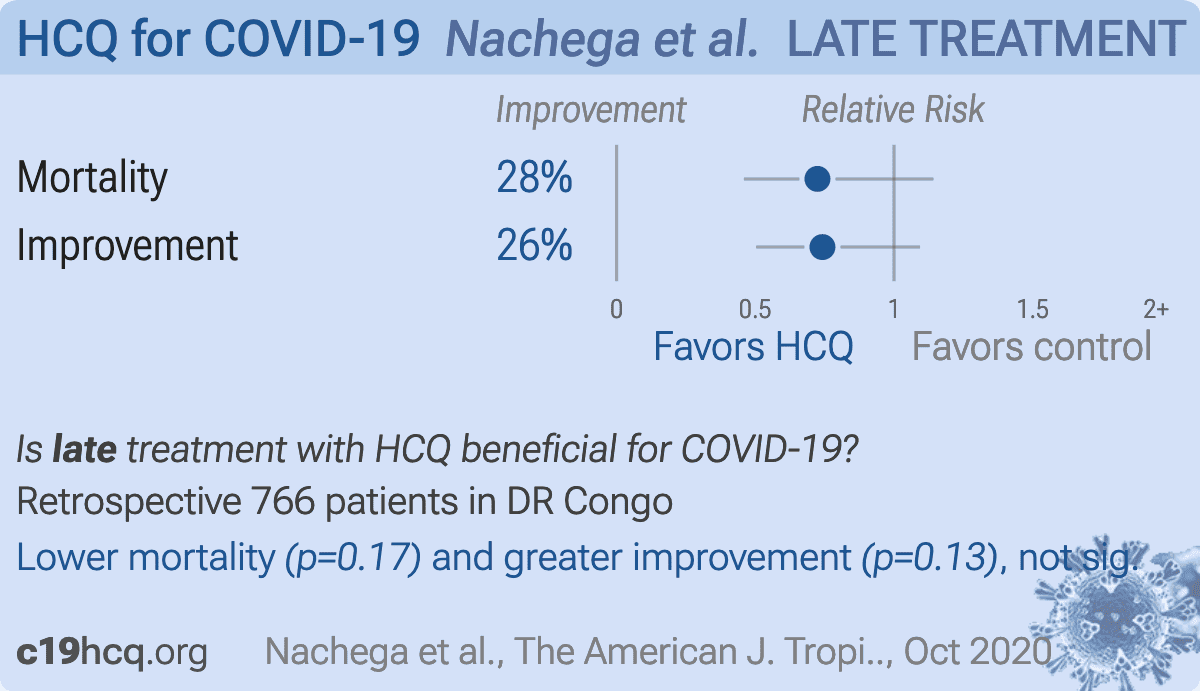
risk of death, 27.6% lower, RR 0.72, p = 0.17, treatment 69 of 630 (11.0%), control 28 of 96 (29.2%), NNT 5.5, adjusted per study, odds ratio converted to relative risk.
|
|
risk of no improvement, 25.8% better, RR 0.74, p = 0.13, adjusted per study, odds ratio converted to relative risk.
|
| Effect extraction follows pre-specified rules prioritizing more serious outcomes. Submit updates |



{kind=link}