Association of subcutaneous or intravenous route of administration of casirivimab and imdevimab monoclonal antibodies with clinical outcomes in COVID-19
PharmD, BCPS, BCIDP Erin K Mccreary, J Ryan Bariola, MD Richard J Wadas, Judith A Shovel, Mary Kay Wisniewski, Michelle Adam, BS Debbie Albin, MS Tami Minnier, MD Mark Schmidhofer, MBA Russell Meyers, MD Oscar C Marroquin, MBA Kevin Collins, PhD William Garrard, Lindsay R Berry, PhD Scott Berry, PhD Amy M Crawford, PhD Anna Mcglothlin, MS Kelsey Linstrum, MS Anna Nakayama, MS Stephanie K Montgomery, MD Graham M Snyder, MD Donald M Yealy, MD MPH Derek C Angus, PhD Paula L Kip, MD MSc Christopher W Seymour, MD MPH David T Huang, PhD Kevin E Kip
doi:10.1101/2021.11.30.21266756
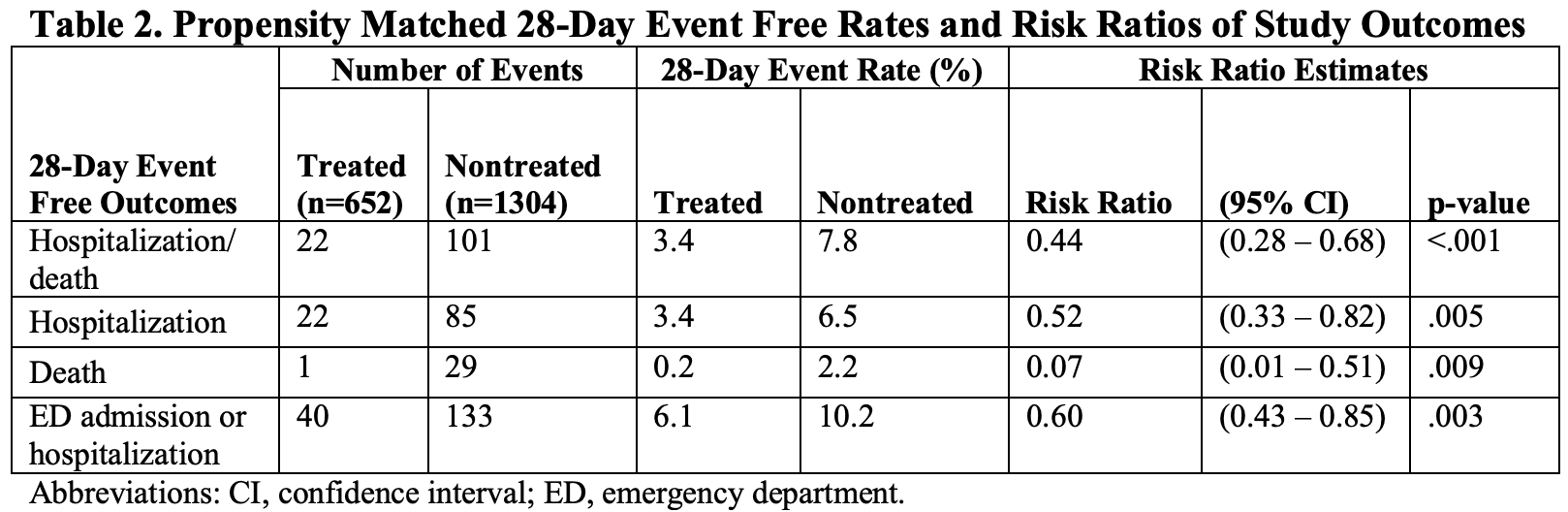
Findings: Among 1,956 propensity-matched adults, outpatients who received casirivimab and imdevimab subcutaneously had a 28-day rate of hospitalization or death of 3.4% (n=652) compared to 7.8% (n=1,304) in non-treated controls [risk ratio 0.44 (95% confidence interval: 0.28 to 0.68, p < .001)]. Among 2,185 outpatients who received subcutaneous (n=969) or intravenous (n=1,216) casirivimab and imdevimab, the 28-day rate of hospitalization/death was 2.8% vs. 1.7%, respectively, which resulted in an adjusted risk difference of 1.5% (95% confidence interval: -0.5% to 3.5%, p=.14). The 28-day adjusted risk differences comparing subcutaneous to intravenous route for death, ICU admission, and mechanical ventilation were 0.3% or less, although the 95% confidence intervals were wide. Meaning: Subcutaneously administered casirivimab and imdevimab is associated with reduced hospitalization or death amongst outpatients with mild to moderate COVID-19 compared to no treatment, and has a small, adjusted risk difference compared to patients treated intravenously.
Treated and Nontreated Analysis
References
Austin, An introduction to propensity score methods for reducing the effects of confounding in observational studies, Multivariate Behav Res,
doi:10.1080/00273171.2011.568786Bariola, Mccreary, Wadas, Impact of bamlanivimab monoclonal antibody treatment on hospitalization and mortality among nonhospitalized adults with severe acute respiratory syndrome coronavirus 2 infection, Open Forum Infect Dis,
doi:10.1093/ofid/ofab254Benchimol, Sl, Guttmann, Harron, The REporting of studies Conducted using Observational Routinely-collected health Data (RECORD) Statement, PLoS Med
Gov, Uk, Patient information leaflet for Ronapreve
Huang, Mccreary, Bariola, The UPMC OPTIMISE-C19 (OPtimizing Treatment and Impact of Monoclonal antIbodieS through Evaluation for COVID-19) trial: a structured summary of a study protocol for an open-label, pragmatic, comparative effectiveness platform trial with response-adaptive randomization, Trials,
doi:10.1186/s13063-021-05316-3O'brien, Forleo-Neto, Musser, Subcutaneous REGEN-COV Antibody Combination to Prevent Covid-19, N Engl J Med,
doi:10.1056/NEJMoa2109682Pfizer, A study of PF-07321332/ritonavir in non-hospitalized low-risk adult participants with COVID-19
Reitz, Seymour, Vates, Strategies to Promote ResiliencY (SPRY): a randomised embedded multifactorial adaptative platform (REMAP) clinical trial protocol to study interventions to improve recovery after surgery in high-risk patients, BMJ Open,
doi:10.1136/bmjopen-2020-037690Rosenbaum, Rubin, The Central Role of the Propensity Score in Observational Studies for Causal Effects, Biometrika,
doi:10.2307/2335942Sharp, Corporation, Efficacy and safety of molnupiravir (MK-4482) in nonhospitalized adult participants with COVID-19


{kind=link}