Inhaled Nitric Oxide via High-Flow Nasal Cannula in Patients with Acute Respiratory Failure Related to COVID-19
Abhimanyu Chandel, Saloni Patolia, Kareem Ahmad, Shambhu Aryal, A Whitney Brown, Dhwani Sahjwani, Vikramjit Khangoora, Oksana A Shlobin, Paula C Cameron, Anju Singhal, Arthur W Holtzclaw, Mehul Desai, Steven D Nathan, Christopher S King
Clinical Medicine Insights: Circulatory, Respiratory and Pulmonary Medicine, doi:10.1177/11795484211047065
INTRODUCTION: Limited evidence exists regarding use of inhaled nitric oxide (iNO) in spontaneously breathing patients. We evaluated the effectiveness of continuous iNO via high-flow nasal cannula (HFNC) in COVID-19 respiratory failure.
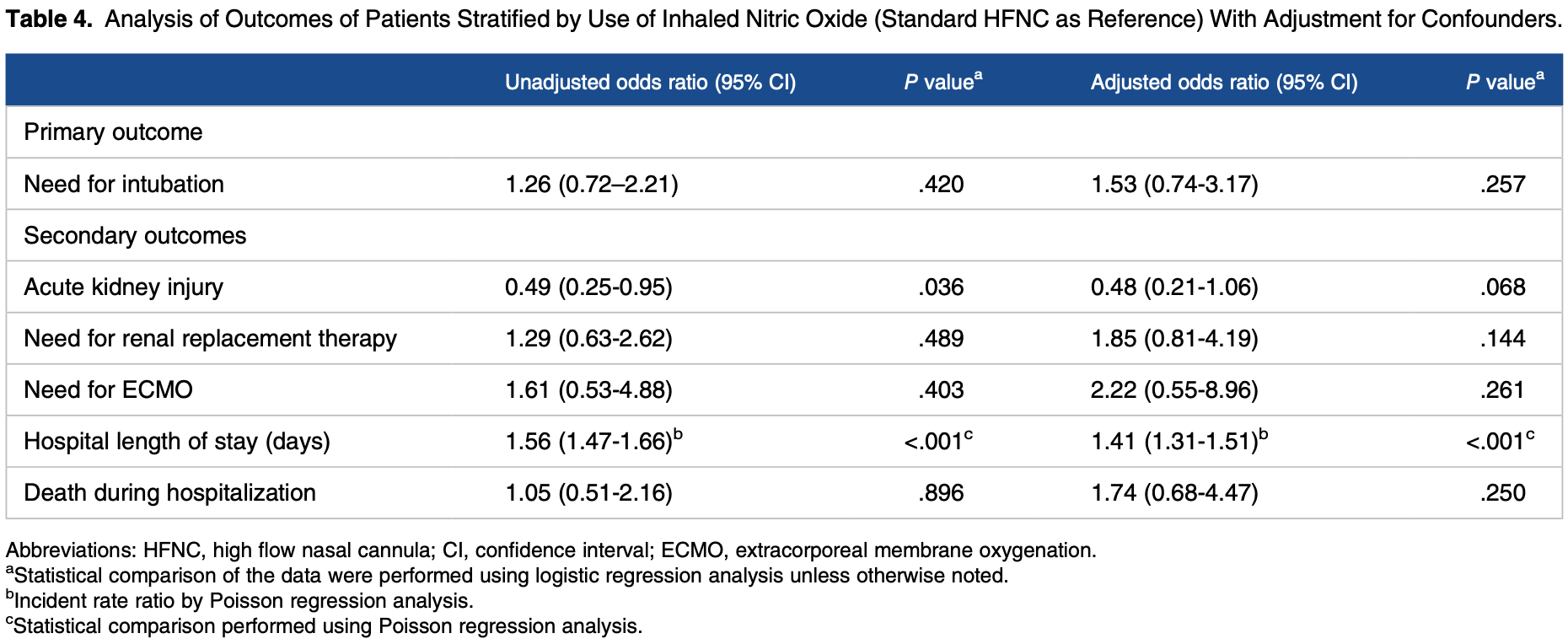
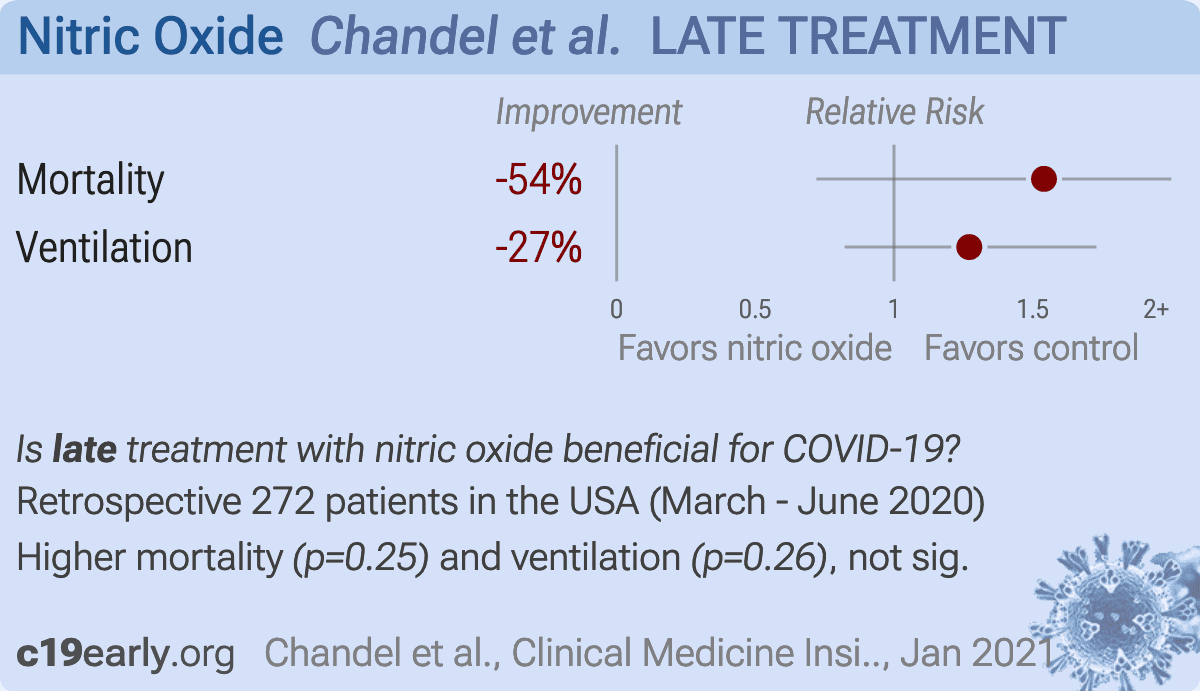
METHODS: We performed a multicenter cohort study of patients with respiratory failure from COVID-19 managed with HFNC. Patients were stratified by administration of iNO via HFNC. Regression analysis was used to compare the need for mechanical ventilation and secondary endpoints including hospital mortality, length of stay, acute kidney injury, need for renal replacement therapy, and need for extracorporeal life support. RESULTS: A total of 272 patients were identified and 66 (24.3%) of these patients received iNO via HFNC for a median of 88 h (interquartile range: 44, 135). After 12 h of iNO, supplemental oxygen requirement was unchanged or increased in 52.7% of patients. Twenty-nine (43.9%) patients treated with iNO compared to 79 (38.3%) patients without iNO therapy required endotracheal intubation (P = .47). After multivariable adjustment, there was no difference in need for mechanical ventilation between groups (odds ratio: 1.53; 95% confidence interval [CI]: 0.74-3.17), however, iNO administration was associated with longer hospital length of stay (incidence rate ratio: 1.41; 95% CI: 1.31-1.51). No difference was found for mortality, acute kidney injury, need for renal replacement therapy, or need for extracorporeal life support.
CONCLUSION: In patients with COVID-19 respiratory failure, iNO delivered via HFNC did not reduce oxygen requirements in the majority of patients or improve clinical outcomes. Given the observed association with increased length of stay, judicious selection of those likely to benefit from this therapy is warranted.
Author Contributions AC and CSK are the guarantors of the content of the manuscript and contributed to all aspects of the project. SP, KA, SA, AWB, DS, VK, OAS, AS, AWH, MD, and SDN contributed substantially to project design, data collection, and
ORCID iD Abhimanyu Chandel https://orcid.org/0000-0003-4879-1983
References
Abou-Arab, Huette, Debouvries, Inhaled nitric oxide for critically ill Covid-19 patients: a prospective study, Crit Care,
doi:10.1186/s13054-020-03371-xAdhikari, Dellinger, Lundin, Inhaled nitric oxide does not reduce mortality in patients with acute respiratory distress syndrome regardless of severity: systematic review and meta-analysis, Crit Care Med,
doi:10.1097/CCM.0b013e3182a27909Akerstrom, Mousavi-Jazi, Klingstrom, Nitric oxide inhibits the replication cycle of severe acute respiratory syndrome coronavirus, J Virol,
doi:10.1128/JVI.79.3.1966-1969.2005Bagate, Tuffet, Masi, Rescue therapy with inhaled nitric oxide and almitrine in COVID-19 patients with severe acute respiratory distress syndrome, Ann Intensive Care,
doi:10.1186/s13613-020-00769-2Berger, Kunichoff, Adhikari, Prevalence and outcomes of D-dimer elevation in hospitalized patients with COVID-19, Arterioscler Thromb Vasc Biol,
doi:10.1161/ATVBAHA.120.314872Chandel, Patolia, Brown, High-flow nasal cannula in COVID-19: outcomes of application and examination of the ROX index to predict success, Respir Care,
doi:10.4187/respcare.08631Chang, Elhusseiny, Yeh, COVID-19 ICU and mechanical ventilation patient characteristics and outcomes-A systematic review and meta-analysis, PLoS ONE,
doi:10.1371/journal.pone.0246318Davis, Crow, Fan, Use and costs of inhaled nitric oxide and inhaled epoprostenol in adult critically ill patients: a quality improvement project, Am J Health Syst Pharm,
doi:10.1093/ajhp/zxz151Dellinger, Zimmerman, Taylor, Effects of inhaled nitric oxide in patients with acute respiratory distress syndrome: results of a randomized phase II trial. Inhaled nitric oxide in ARDS study group, Crit Care Med,
doi:10.1097/00003246-199801000-00011Demoule, Baron, Darmon, High-flow nasal cannula in critically III patients with severe COVID-19, Am J Respir Crit Care Med,
doi:10.1164/rccm.202005-2007LEEly, Shintani, Monitoring sedation status over time in ICU patients: reliability and validity of the Richmond Agitation-Sedation Scale (RASS), JAMA,
doi:10.1001/jama.289.22.2983Gattinoni, Coppola, Cressoni, COVID-19 does not lead to a "typical" acute respiratory distress syndrome, Am J Respir Crit Care Med,
doi:10.1164/rccm.202003-0817LEGebistorf, Karam, Wetterslev, Inhaled nitric oxide for acute respiratory distress syndrome (ARDS) in children and adults, Cochrane Database Syst Rev,
doi:10.1002/14651858.CD002787.pub3Kline, Puskarich, Jones, Inhaled nitric oxide to treat intermediate risk pulmonary embolism: a multicenter randomized controlled trial, Nitric Oxide,
doi:10.1016/j.niox.2019.01.006Longobardo, Montanari, Shulman, Inhaled nitric oxide minimally improves oxygenation in COVID-19 related acute respiratory distress syndrome, Br J Anaesth,
doi:10.1016/j.bja.2020.10.011Nishimura, High-flow nasal cannula oxygen therapy in adults: physiological benefits, indication, clinical benefits, and adverse effects, Respir Care,
doi:10.4187/respcare.04577Parikh, Wilson, Weinberg, Inhaled nitric oxide treatment in spontaneously breathing COVID-19 patients, Ther Adv Respir Dis,
doi:10.1177/1753466620933510Reynolds, Lee, Renz, Pulmonary vascular dilatation detected by automated transcranial Doppler in COVID-19 pneumonia, Am J Respir Crit Care Med,
doi:10.1164/rccm.202006-2219LETavazzi, Pozzi, Mongodi, Inhaled nitric oxide in patients admitted to intensive care unit with COVID-19 pneumonia, Crit Care,
doi:10.1186/s13054-020-03222-9Therapeutics, Bellerophon Therapeutics Announces Results of Interim Analysis of Phase 3 COViNOX Study of INOpulse® for the Treatment of COVID-19
Tzanetos, Housley, Barr, Implementation of an inhaled nitric oxide protocol decreases direct cost associated with its use, Respir Care,
doi:10.4187/respcare.03308Wiegand, Fakhr, Carroll, Rescue treatment with high-dose gaseous nitric oxide in spontaneously breathing patients with severe coronavirus disease 2019, Crit Care Explor,
doi:10.1097/cce.0000000000000277


{kind=link}