|
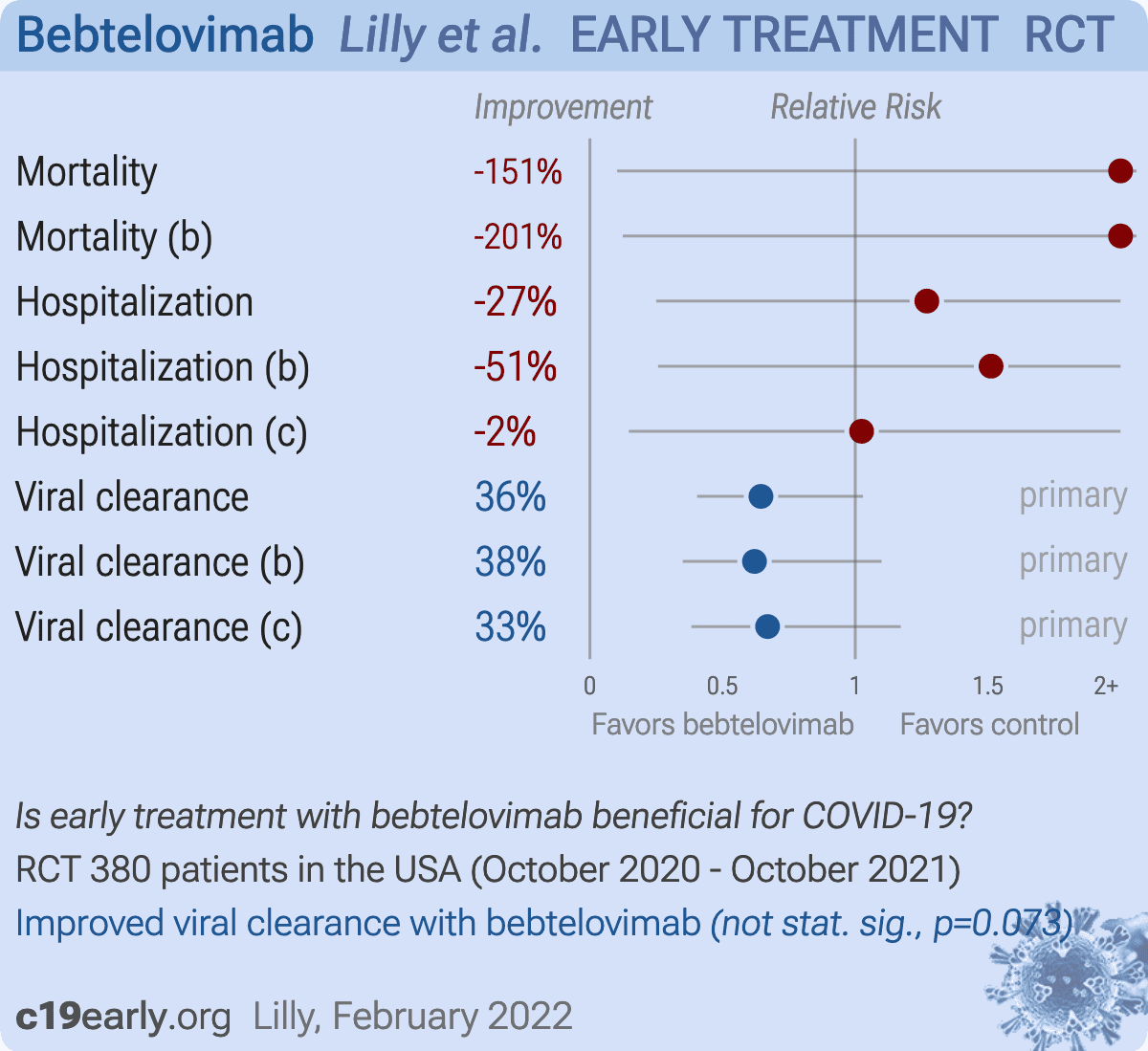
risk of death, 150.8% higher, RR 2.51, p = 1.00, treatment 1 of 252 (0.4%), control 0 of 128 (0.0%), continuity correction due to zero event (with reciprocal of the contrasting arm), combined bebtelovimab arms.
|
|
risk of death, 200.8% higher, RR 3.01, p = 0.50, treatment 1 of 127 (0.8%), control 0 of 128 (0.0%), continuity correction due to zero event (with reciprocal of the contrasting arm), bamlanivimab, etesevimab, and bebtelovimab.
|
|
risk of hospitalization, 27.0% higher, RR 1.27, p = 1.00, treatment 5 of 252 (2.0%), control 2 of 128 (1.6%), combined bebtelovimab arms.
|
|
risk of hospitalization, 51.2% higher, RR 1.51, p = 0.68, treatment 3 of 127 (2.4%), control 2 of 128 (1.6%), bamlanivimab, etesevimab, and bebtelovimab.
|
|
risk of hospitalization, 2.4% higher, RR 1.02, p = 1.00, treatment 2 of 125 (1.6%), control 2 of 128 (1.6%), bebtelovimab.
|
|
risk of no viral clearance, 35.5% lower, RR 0.64, p = 0.07, treatment 33 of 252 (13.1%), control 26 of 128 (20.3%), NNT 14, day 7 persistently high viral load, combined bebtelovimab arms, primary outcome.
|
|
risk of no viral clearance, 38.0% lower, RR 0.62, p = 0.13, treatment 16 of 127 (12.6%), control 26 of 128 (20.3%), NNT 13, day 7 persistently high viral load, bamlanivimab, etesevimab, and bebtelovimab, primary outcome.
|
|
risk of no viral clearance, 33.0% lower, RR 0.67, p = 0.18, treatment 17 of 125 (13.6%), control 26 of 128 (20.3%), NNT 15, day 7 persistently high viral load, bebtelovimab, primary outcome.
|
| Effect extraction follows pre-specified rules prioritizing more serious outcomes. Submit updates |


{kind=link}
{kind=link}